

A retrospective analysis of the effects of different analgesics on the pain of patients with traumatic thoracolumbar fractures in the peri-treatment period
- PMID: 33865404
- PMCID: PMC8052732
- DOI: 10.1186/s13018-021-02401-w
A retrospective analysis of the effects of different analgesics on the pain of patients with traumatic thoracolumbar fractures in the peri-treatment period
Abstract
Objective: To analyze and compare the effects of peri-treatment analgesics on acute and chronic pain and postoperative functional recovery of patients with thoracolumbar fractures, so as to guide the clinical drug use.
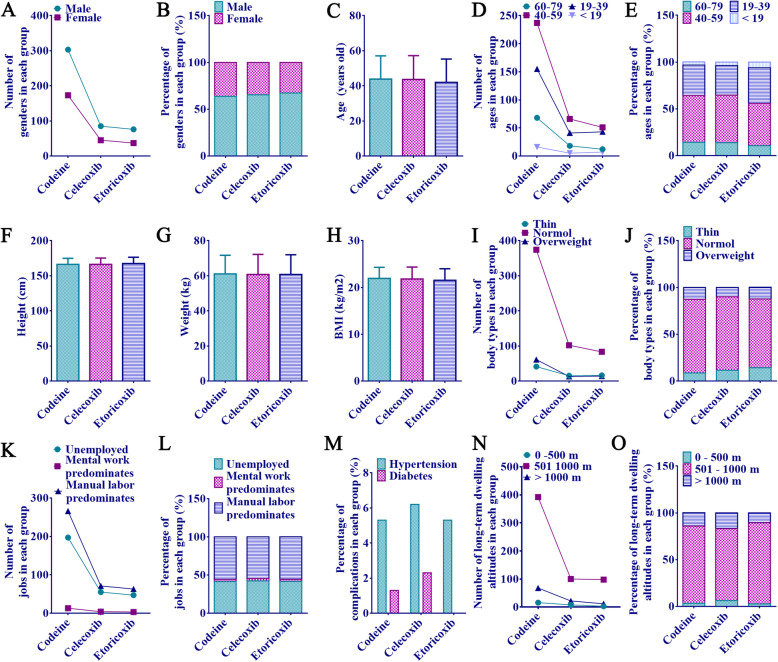
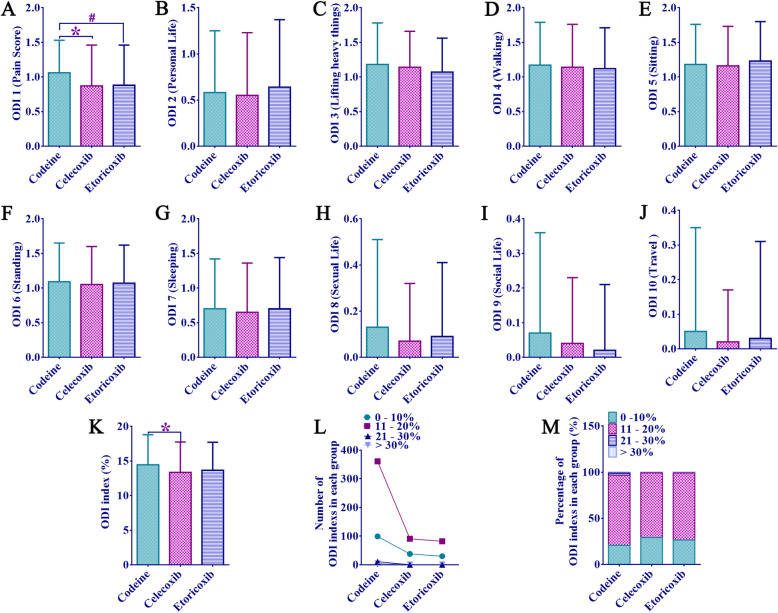
Methods: Seven hundred nineteen patients with thoracolumbar fractures were collected and divided into acetaminophen dihydrocodeine, celecoxib, and etoricoxib groups. The main indicators were the degree of postoperative pain (visual analog scale (VAS)), the incidence of chronic pain and postoperative functional recovery (Oswestry dysfunction index (ODI) and Japanese Orthopedics Association score (JOA)), which were continuously tracked through long-term telephone follow-up. The correlation analysis of ODI-pain score, peri-treatment VAS score, and ODI index was performed, and bivariate regression analysis was conducted to understand the risk factors for chronic pain.
Results: Regression analysis showed that severe spinal cord injury and peri-treatment use of acetaminophen dihydrocodeine were both one of the risk factors for postoperative chronic pain. But there were no statistically conspicuous differences in basic characteristics, preoperative injury, and intraoperative conditions. Compared with the other two groups, patients in the acetaminophen dihydrocodeine group had longer peri-therapeutic analgesic use, higher pain-related scores (VAS 1 day preoperatively, VAS 1 month postoperatively, and ODI-pain 1 year postoperatively), higher VAS variation, higher incidence of chronic pain 1 year after surgery, and higher ODI index. And other ODI items and JOA assessments showed no statistically significant differences. In addition, the correlation analysis showed that the peri-treatment pain score was correlated with the severity of postoperative chronic pain.
Conclusion: Although the peri-treatment analgesic effect of acetaminophen dihydrocodeine is good, it is still necessary to combine analgesics with different mechanisms of action for patients with severe preoperative pain of thoracolumbar fracture, so as to inhibit the incidence of postoperative chronic pain and improve the quality of postoperative rehabilitation.
Keywords: Acetaminophen dihydrocodeine; Celecoxib; Etoricoxib; Pain degree; Traumatic thoracolumbar fracture.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures


References
-
- Liu P, Yao Y, Liu MY, Fan WL, Chao R, Wang ZG, Liu YC, Zhou JH, Zhao JH Spinal trauma in mainland China from 2001 to 2007: an epidemiological study based on a nationwide database. Spine (Phila Pa 1976). 2012;37(15):1310-1315. Epub 2012/06/30. doi: 10.1097/BRS.0b013e3182474d8b. PubMed PMID: 22744399. - PubMed
-
- Wood KB, Li W, Lebl DR, Ploumis A. Management of thoracolumbar spine fractures. Spine J. 2014;14(1):145-164. Epub 2013/12/18. doi: 10.1016/j.spinee.2012.10.041. PubMed PMID: 24332321. - PubMed
-
- Graham GG, Scott KF. Mechanism of action of paracetamol. Am J Ther. 2005;12(1):46-55. Epub 2005/01/22. doi: 10.1097/00045391-200501000-00008. PubMed PMID: 15662292. - PubMed
-
- Esmailian M, Moshiri R, Zamani M. Comparison of the analgesic effect of intravenous acetaminophen and morphine sulfate in rib fracture; a randomized double-blind clinical trial. Emergency (Tehran, Iran). 2015;3(3):99-102. Epub 2015/10/27. PubMed PMID: 26495393; PubMed Central PMCID: PMCPMC4608332. - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
