

Adjuvant tegafur-uracil (UFT) or S-1 monotherapy for advanced gastric cancer: a single center experience
- PMID: 33865416
- PMCID: PMC8053033
- DOI: 10.1186/s12957-021-02233-2
Adjuvant tegafur-uracil (UFT) or S-1 monotherapy for advanced gastric cancer: a single center experience
Abstract
Background: Adjuvant tegafur-gimeracil-oteracil (S-1) is commonly used for gastric cancer in Asia, and tegafur-uracil (UFT) is another oral fluoropyrimidine when S-1 is unavailable. The real-world data of adjuvant UFT has less been investigated.
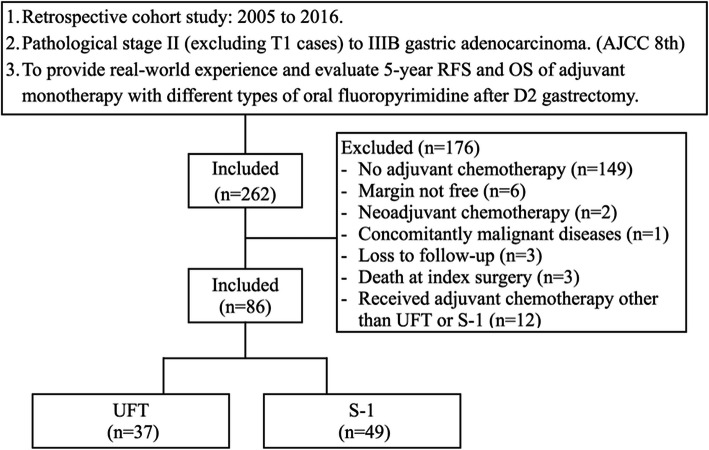
Methods: Patients with pathological stage II-IIIB (except T1) gastric cancer receiving adjuvant UFT or S-1 monotherapy after D2 gastrectomy were included. Usage of UFT or S-1 was based on reimbursement policy of the Taiwanese healthcare system. The characteristics, chemotherapy completion rates, and 5-year recurrence-free survival (RFS) and overall survival (OS), were compared between these two groups.
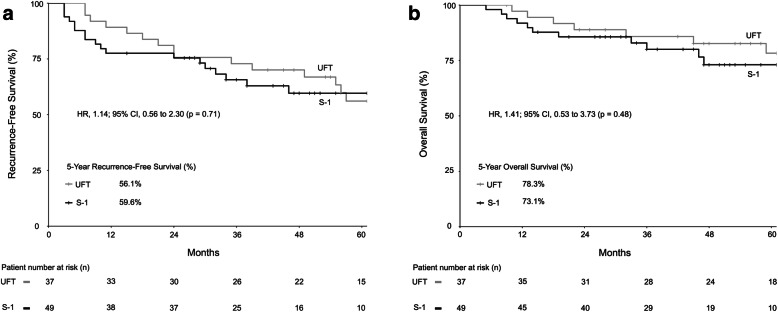
Results: From 2005 to 2016, 86 eligible patients were included. Most tumor characteristics were similar between the UFT group (n = 37; age 59.1 ± 13.9 years) and S-1 group (n = 49; age 56.3 ± 10.7 years), except there were significantly more Borrmann type III/IV (86.5% versus 67.3%; p = 0.047) and T4 (56.8% versus 10.2%; p < 0.001) lesions in the UFT group than in the S-1 group. The chemotherapy complete rates were similar in the two groups. The 5-year RFS was 56.1% in the UFT group and 59.6% in the S-1 group (p = 0.71), and the 5-year OS was 78.3% in the UFT group and 73.1% in the S-1 group (p = 0.48). The hazard ratio of adjuvant chemotherapy (S-1 versus UFT) on RFS was 1.25 (95% confidence interval = 0.53-2.94) when Borrmann type and T and N stages were adjusted.
Conclusions: This small cohort study showed adjuvant UFT, and S-1 monotherapy had a comparable long-term outcome for pathological stage II-IIIB gastric cancer following D2 gastrectomy.
Keywords: Adjuvant chemotherapy; Gastric cancer; S-1; Tegafur; UFT.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Bang YJ, Kim YW, Yang HK, Chung HC, Park YK, Lee KH, Lee KW, Kim YH, Noh SI, Cho JY, Mok YJ, Kim YH, Ji J, Yeh TS, Button P, Sirzén F, Noh SH. Adjuvant capecitabine and oxaliplatin for gastric cancer after D2 gastrectomy (CLASSIC): a phase 3 open-label, randomised controlled trial. Lancet. 2012;379(9813):315–321. doi: 10.1016/S0140-6736(11)61873-4. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
