

A randomized, double-blind, phase 2b proof-of-concept clinical trial in early Alzheimer's disease with lecanemab, an anti-Aβ protofibril antibody
- PMID: 33865446
- PMCID: PMC8053280
- DOI: 10.1186/s13195-021-00813-8
A randomized, double-blind, phase 2b proof-of-concept clinical trial in early Alzheimer's disease with lecanemab, an anti-Aβ protofibril antibody
Erratum in
-
Correction to: A randomized, double-blind, phase 2b proof-of-concept clinical trial in early Alzheimer's disease with lecanemab, an anti-Aβ protofibril antibody.Alzheimers Res Ther. 2022 May 21;14(1):70. doi: 10.1186/s13195-022-00995-9. Alzheimers Res Ther. 2022. PMID: 35598024 Free PMC article. No abstract available.
Abstract
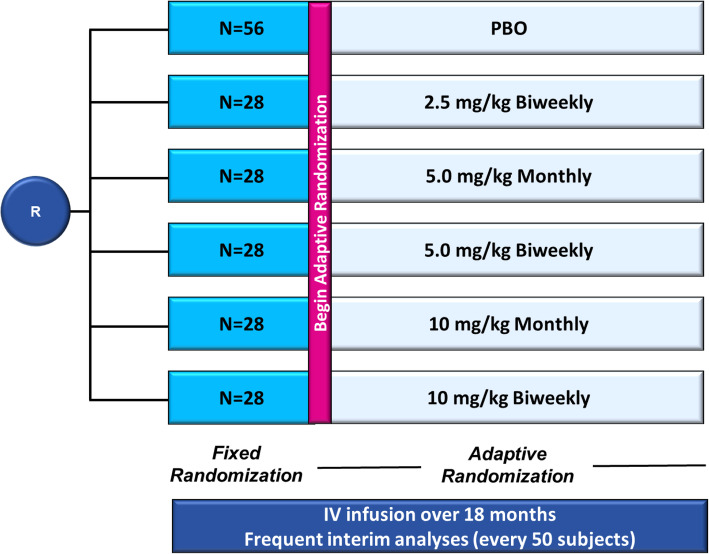
Background: Lecanemab (BAN2401), an IgG1 monoclonal antibody, preferentially targets soluble aggregated amyloid beta (Aβ), with activity across oligomers, protofibrils, and insoluble fibrils. BAN2401-G000-201, a randomized double-blind clinical trial, utilized a Bayesian design with response-adaptive randomization to assess 3 doses across 2 regimens of lecanemab versus placebo in early Alzheimer's disease, mild cognitive impairment due to Alzheimer's disease (AD) and mild AD dementia.
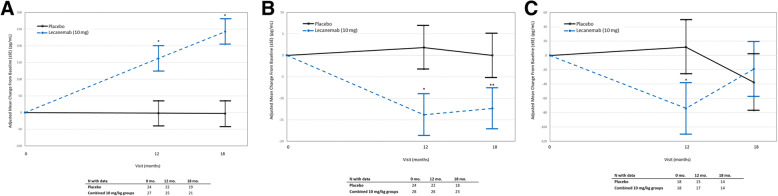
Methods: BAN2401-G000-201 aimed to establish the effective dose 90% (ED90), defined as the simplest dose that achieves ≥90% of the maximum treatment effect. The primary endpoint was Bayesian analysis of 12-month clinical change on the Alzheimer's Disease Composite Score (ADCOMS) for the ED90 dose, which required an 80% probability of ≥25% clinical reduction in decline versus placebo. Key secondary endpoints included 18-month Bayesian and frequentist analyses of brain amyloid reduction using positron emission tomography; clinical decline on ADCOMS, Clinical Dementia Rating-Sum-of-Boxes (CDR-SB), and Alzheimer's Disease Assessment Scale-Cognitive Subscale (ADAS-Cog14); changes in CSF core biomarkers; and total hippocampal volume (HV) using volumetric magnetic resonance imaging.
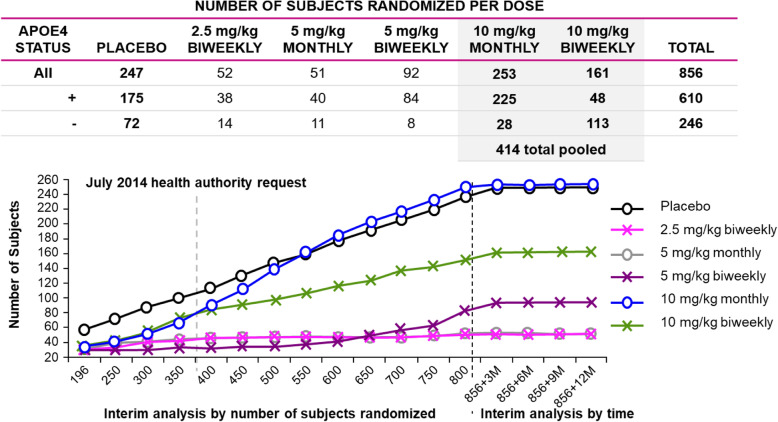
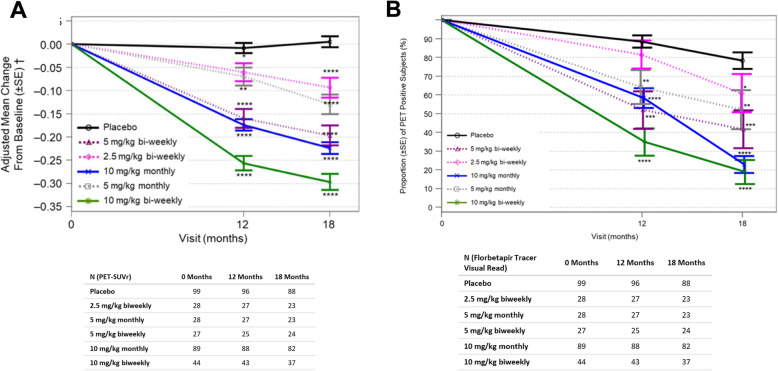
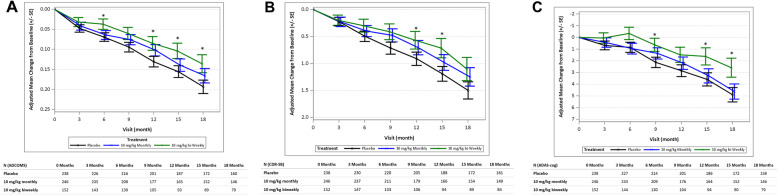
Results: A total of 854 randomized subjects were treated (lecanemab, 609; placebo, 245). At 12 months, the 10-mg/kg biweekly ED90 dose showed a 64% probability to be better than placebo by 25% on ADCOMS, which missed the 80% threshold for the primary outcome. At 18 months, 10-mg/kg biweekly lecanemab reduced brain amyloid (-0.306 SUVr units) while showing a drug-placebo difference in favor of active treatment by 27% and 30% on ADCOMS, 56% and 47% on ADAS-Cog14, and 33% and 26% on CDR-SB versus placebo according to Bayesian and frequentist analyses, respectively. CSF biomarkers were supportive of a treatment effect. Lecanemab was well-tolerated with 9.9% incidence of amyloid-related imaging abnormalities-edema/effusion at 10 mg/kg biweekly.
Conclusions: BAN2401-G000-201 did not meet the 12-month primary endpoint. However, prespecified 18-month Bayesian and frequentist analyses demonstrated reduction in brain amyloid accompanied by a consistent reduction of clinical decline across several clinical and biomarker endpoints. A phase 3 study (Clarity AD) in early Alzheimer's disease is underway.
Trial registration: Clinical Trials.gov NCT01767311 .
Keywords: ADCOMS; Alzheimer’s disease; Amyloid; Amyloid PET; BAN2401; Biomarker; Clinical trial; Lecanemab; Neurofilament light; Neurogranin; p-tau.
Conflict of interest statement
CJS, YZ, SD, JW, JK, RYKL, HB, MR, AK, LR, RG, and LDK are employees of Eisai. LL is an employee of BioArctic. DAB and SB are employees of Berry Consultants. JLC provided consultation to the following pharmaceutical companies: Acadia, Accera, Actinogen, ADAMAS, Alkahest, Allergan, Alzheon, Avanir, Axovant, Axsome, BiOasis Technologies, Biogen, Eisai, Genentech, Grifols, Kyowa, Lilly, Lundbeck, Merck, Nutricia, Otsuka, QR Pharma, Resverlogix, Roche, Samus, Servier, Suven, Takeda, Toyoma, and United Neuroscience companies. JLC is supported by NIGMS grant P20GM109025; NINDS grant U01NS093334; NIA grant R01AG053798; and NIA grant P20AG068053.
Figures
References
-
- Dubois B, Feldman HH, Jacova C, Cummings JL, DeKosky ST, Barberger-Gateau P, Delacourte A, Frisoni G, Fox NC, Galasko D, Gauthier S, Hampel H, Jicha GA, Meguro K, O'Brien J, Pasquier F, Robert P, Rossor M, Salloway S, Sarazin M, de Souza LC, Stern Y, Visser PJ, Scheltens P. Revising the definition of Alzheimer’s disease: a new lexicon. Lancet Neurol. 2010;9(11):1118–1127. doi: 10.1016/S1474-4422(10)70223-4. - DOI - PubMed
-
- Masters C, Bateman R, Blennow K, et al. Alzheimer’s disease. Nat Rev. 2015;1:15056. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
