

Potts shunt as an effective palliation for patients with end stage pulmonary arterial hypertension
- PMID: 33865518
- PMCID: PMC8065372
- DOI: 10.1016/j.ihj.2021.01.007
Potts shunt as an effective palliation for patients with end stage pulmonary arterial hypertension
Abstract
Background: Potts shunt has been suggested as an effective palliative therapy for patients with pulmonary artery hypertension (PAH) not associated with congenital heart disease.
Materials and methods: This is a prospective single-center study performed to assess outcomes of Potts shunt in patients with PAH who are in functional class III or IV.
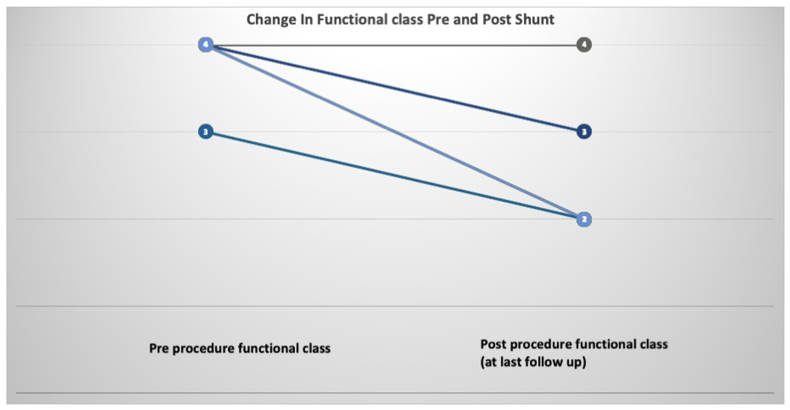
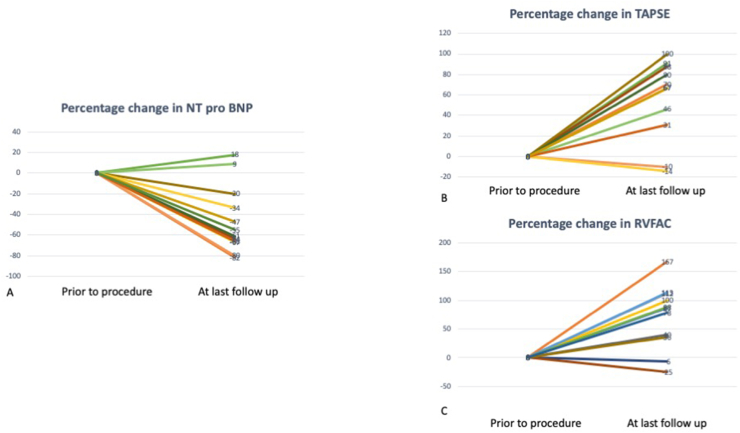
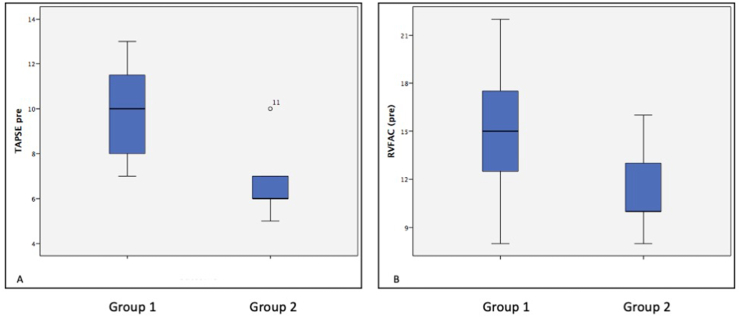
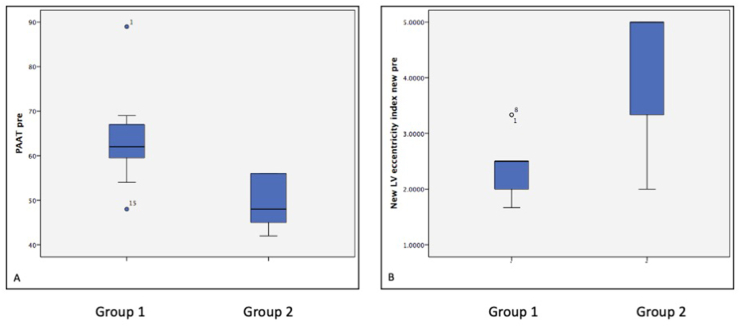
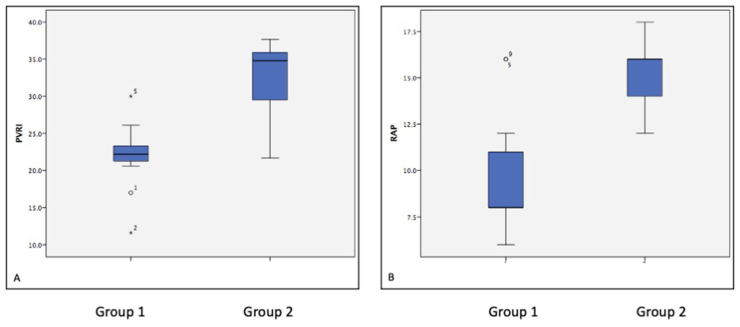
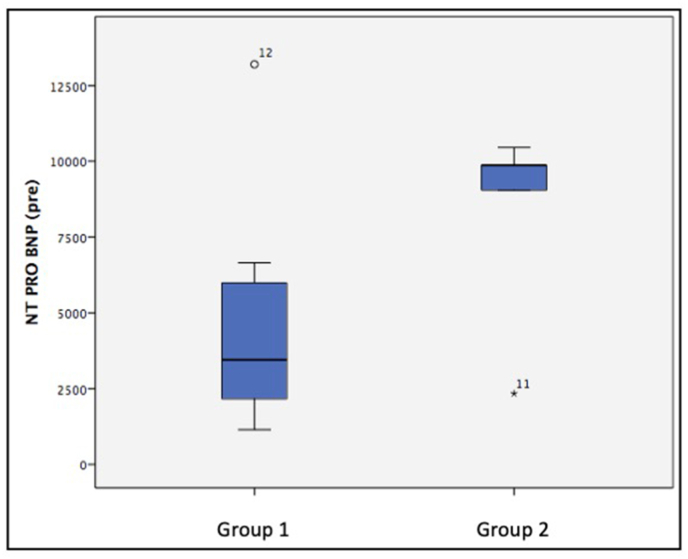
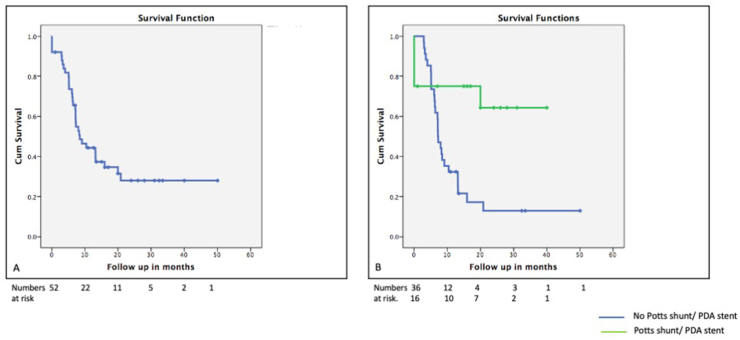
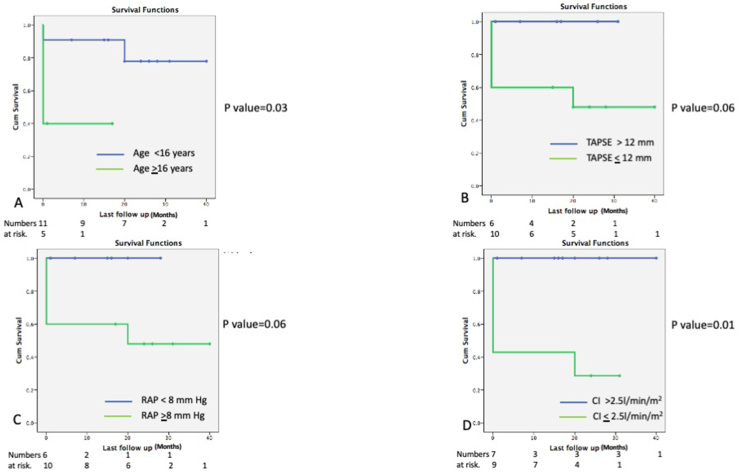
Results: 52 patients in functional class III/IV with pulmonary arterial hypertension without significant intra or extracardiac shunt on maximal medical therapy were evaluated and counseled for undergoing Potts shunt/patent ductus arteriosus (PDA) stenting. 16/52 patients (13 females) consented for the procedure; 14 patients underwent surgical creation of Potts, and 2 underwent transcatheter stenting of PDA, which physiologically acted like a Potts shunt. Standard medical therapy was continued in patients who did not consent for the procedure. 12/16 patients survived the procedure. Patients who did not survive the procedure were older, with severe right ventricular systolic dysfunction, and functional class IV. Patients who survived the procedure were followed up in the pulmonary hypertension clinic. The Median follow-up was 17 months (1-40 months). 11/13 patients discharged after the operation showed sustained clinical, echocardiographic, and biochemical improvement, which reduced need for pulmonary vasodilator therapy in 10/13 patients. There was one death in the follow-up period 16 months post-surgery due to lower respiratory tract infection.
Conclusion: Potts shunt is feasible in patients with PAH without significant intra or extracardiac shunts. It can be done safely with an acceptable success rate. Patient selection, preoperative stabilization, and meticulous postoperative management are essential. It should be performed at the earliest sign of clinical, echocardiographic, or laboratory deterioation for optimal outcomes. Long-term follow-up is required to see a sustained improvement in functional class and the need for a lung transplant in the future.
Keywords: Bridge to transplant; Reverse Potts shunt; Right ventricular dysfunction.
Copyright © 2021 Cardiological Society of India. Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
Declaration of competing interest None.
Figures
Similar articles
-
Reversed Potts Shunt Outcome in Suprasystemic Pulmonary Arterial Hypertension: A Systematic Review and Meta-Analysis.Curr Cardiol Rev. 2022;18(6):e090522204486. doi: 10.2174/1573403X18666220509203335. Curr Cardiol Rev. 2022. PMID: 35538823 Free PMC article.
-
Palliative Potts shunt for the treatment of children with drug-refractory pulmonary arterial hypertension: updated data from the first 24 patients.Eur J Cardiothorac Surg. 2015 Mar;47(3):e105-10. doi: 10.1093/ejcts/ezu445. Epub 2014 Dec 4. Eur J Cardiothorac Surg. 2015. PMID: 25475943
-
Potts shunt in children with idiopathic pulmonary arterial hypertension: long-term results.Ann Thorac Surg. 2012 Sep;94(3):817-24. doi: 10.1016/j.athoracsur.2012.03.099. Epub 2012 Jun 15. Ann Thorac Surg. 2012. PMID: 22704329
-
Midterm outcomes of the Potts shunt for pediatric pulmonary hypertension, with comparison to lung transplant.J Thorac Cardiovasc Surg. 2021 Mar;161(3):1139-1148. doi: 10.1016/j.jtcvs.2020.10.163. Epub 2020 Dec 9. J Thorac Cardiovasc Surg. 2021. PMID: 33454101
-
Beyond transplant: Roles of atrial septostomy and Potts shunt in pediatric pulmonary hypertension.Pediatr Pulmonol. 2021 Mar;56(3):656-660. doi: 10.1002/ppul.25049. Epub 2020 Sep 11. Pediatr Pulmonol. 2021. PMID: 32860488 Review.
Cited by
-
Perioperative Echocardiographic Management of a Surgical Right Pulmonary Artery-Left Atrial Shunt as a Bridge to Lung Transplantation.CASE (Phila). 2025 Apr 1;9(6):187-193. doi: 10.1016/j.case.2025.02.003. eCollection 2025 Jun. CASE (Phila). 2025. PMID: 40583872 Free PMC article.
-
Cardiopulmonary Exercise Testing With Forehead and Popliteal Oximetry in Evaluating Efficacy of Reverse Potts Shunt.JACC Case Rep. 2025 Apr 2;30(7):103409. doi: 10.1016/j.jaccas.2025.103409. JACC Case Rep. 2025. PMID: 40185583 Free PMC article.
-
Long-term outcomes of transcatheter Potts shunt in children with suprasystemic pulmonary arterial hypertension.Front Cardiovasc Med. 2022 Oct 26;9:1028304. doi: 10.3389/fcvm.2022.1028304. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 36386337 Free PMC article.
-
Reversed Potts Shunt Outcome in Suprasystemic Pulmonary Arterial Hypertension: A Systematic Review and Meta-Analysis.Curr Cardiol Rev. 2022;18(6):e090522204486. doi: 10.2174/1573403X18666220509203335. Curr Cardiol Rev. 2022. PMID: 35538823 Free PMC article.
-
Interventional Strategies for Children with Progressive Pulmonary Hypertension Despite Optimal Therapy: An Official American Thoracic Society Clinical Practice Guideline.Am J Respir Crit Care Med. 2025 Feb;211(2):157-173. doi: 10.1164/rccm.202410-1901ST. Am J Respir Crit Care Med. 2025. PMID: 39531626 Free PMC article.
References
-
- Ivy D.D., Abman S.H., Barst R.J. Pediatric pulmonary hypertension. J Am Coll Cardiol. 2013;62(25 Suppl):D117–D126. - PubMed
-
- Goldstein B.S., Sweet S.C., Mao J., Huddleston C.B., Grady R.M. Lung transplantation in children with idiopathic pulmonary arterial hypertension: an 18-year experience. J Heart Lung Transplant. 2011;30(10):1148–1152. - PubMed
-
- Baruteau A.E., Belli E., Boudjemline Y. Palliative Potts shunt for the treatment of children with drug-refractory pulmonary arterial hypertension: updated data from the first 24 patients. Eur J Cardio Thorac Surg. 2015;47(3):e105–e110. - PubMed
-
- Keogh A.M., Nicholls M., Shaw M., Dhital K., Weintraub R., Winlaw D.S. Modified Potts shunt in an adult with pulmonary arterial hypertension and recurrent syncope - three-year follow-up. Int J Cardiol. 2015;182:36–37. - PubMed
-
- Hopkins W.E., Waggoner A.D. Severe pulmonary hypertension without right ventricular failure: the unique hearts of patients with Eisenmenger syndrome. Am J Cardiol. 2002;89(1):34–38. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
