

Relationships between preoperative cortical thickness, postoperative electroencephalogram slowing, and postoperative delirium
- PMID: 33865555
- PMCID: PMC8442560
- DOI: 10.1016/j.bja.2021.02.028
Relationships between preoperative cortical thickness, postoperative electroencephalogram slowing, and postoperative delirium
Abstract
Background: It is unclear how preoperative neurodegeneration and postoperative changes in EEG delta power relate to postoperative delirium severity. We sought to understand the relative relationships between neurodegeneration and delta power as predictors of delirium severity.
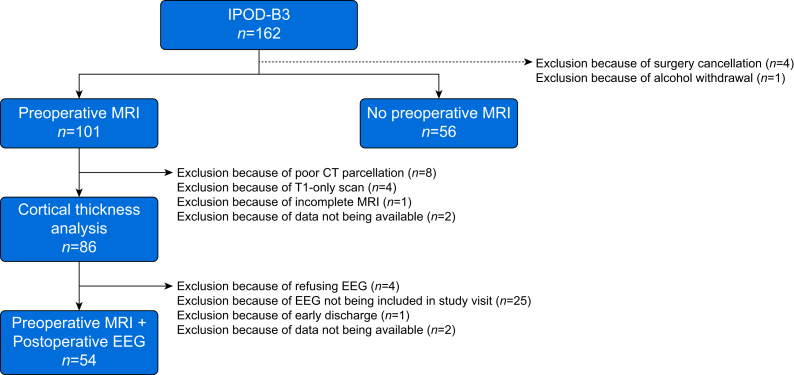
Methods: We undertook a prospective cohort study of high-risk surgical patients (>65 yr old) to identify predictors of peak delirium severity (Delirium Rating Scale-98) with twice-daily delirium assessments (NCT03124303). Participants (n=86) underwent preoperative MRI; 54 had both an MRI and a postoperative EEG. Cortical thickness was calculated from the MRI and delta power from the EEG.
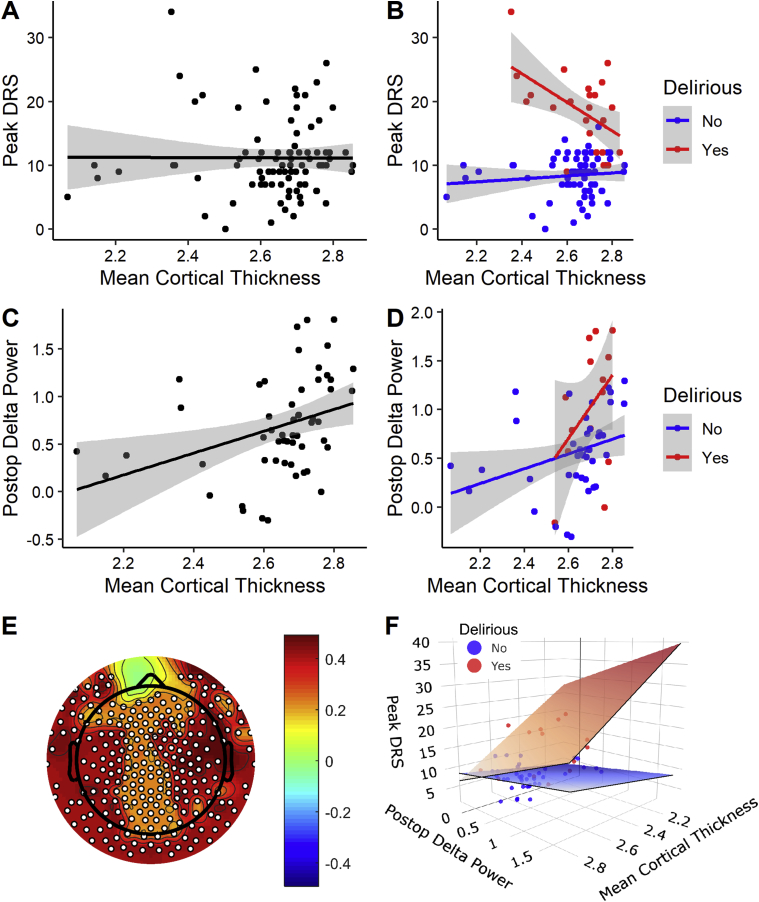
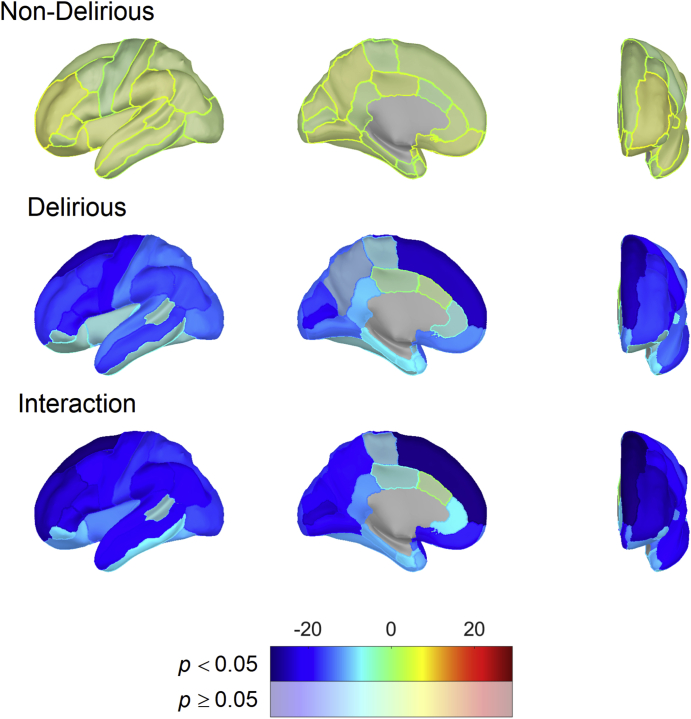
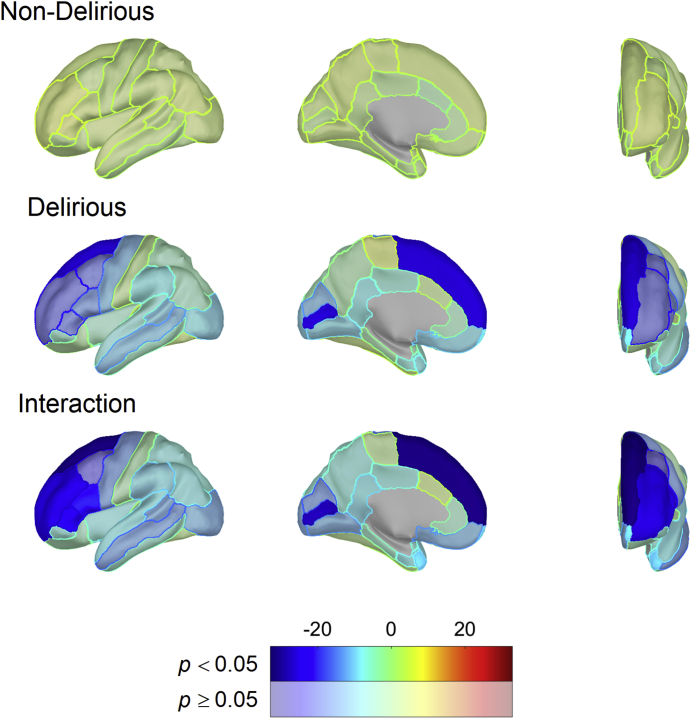
Results: In a linear regression model, the interaction between delirium status and preoperative mean cortical thickness (suggesting neurodegeneration) across the entire cortex was a significant predictor of delirium severity (P<0.001) when adjusting for age, sex, and performance on preoperative Trail Making Test B. Next, we included postoperative delta power and repeated the analysis (n=54). Again, the interaction between mean cortical thickness and delirium was associated with delirium severity (P=0.028), as was postoperative delta power (P<0.001). When analysed across the Desikan-Killiany-Tourville atlas, thickness in multiple individual cortical regions was also associated with delirium severity.
Conclusions: Preoperative cortical thickness and postoperative EEG delta power are both associated with postoperative delirium severity. These findings might reflect different underlying processes or mechanisms.
Clinical trial registration: NCT03124303.
Keywords: cortical slowing; cortical thickness; delirium; neurodegeneration; surgery.
Copyright © 2021 British Journal of Anaesthesia. Published by Elsevier Ltd. All rights reserved.
Figures
References
-
- Witlox J., Eurelings L.S., de Jonghe J.F., Kalisvaart K.J., Eikelenboom P., van Gool W.A. Delirium in elderly patients and the risk of postdischarge mortality, institutionalization, and dementia: a meta-analysis. JAMA. 2010;304:443–451. - PubMed
-
- Sanders R.D., Pandharipande P.P., Davidson A.J., Ma D., Maze M. Anticipating and managing postoperative delirium and cognitive decline in adults. BMJ. 2011;343:d4331. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
