

Cost-effectiveness of sequential daily teriparatide/weekly alendronate compared with alendronate monotherapy for older osteoporotic women with prior vertebral fracture in Japan
- PMID: 33866457
- PMCID: PMC8053143
- DOI: 10.1007/s11657-021-00891-z
Cost-effectiveness of sequential daily teriparatide/weekly alendronate compared with alendronate monotherapy for older osteoporotic women with prior vertebral fracture in Japan
Abstract
Using a Markov microsimulation model among hypothetical cohorts of community-dwelling older osteoporotic Japanese women with prior vertebral fracture over a lifetime horizon, we found that daily subcutaneous teriparatide for 2 years followed by weekly oral alendronate for 8 years was not cost-effective compared with alendronate monotherapy for 10 years.
Purpose: Teriparatide has proven efficacy in reducing osteoporotic fractures, but with substantial cost. We examined the cost-effectiveness of sequential teriparatide/alendronate (i.e., daily subcutaneous teriparatide for 2 years followed by weekly oral alendronate for 8 years) compared with alendronate monotherapy for 10 years among community-dwelling older osteoporotic women with prior clinical or morphometric vertebral fracture in Japan.
Methods: Using a previously validated and updated Markov microsimulation model, we obtained incremental cost-effectiveness ratios (Japanese yen [¥] (or US dollars [$]) per quality-adjusted life year [QALY]) from the perspective of a single payer responsible for both public healthcare and long-term care. We assumed a lifetime horizon with a willingness-to-pay of ¥5million (or $47,500) per QALY in the base case. We modeled the cost of biosimilar teriparatide, which has been available since November 2019 in Japan, assuming the efficacy was the same as that of the brand version.
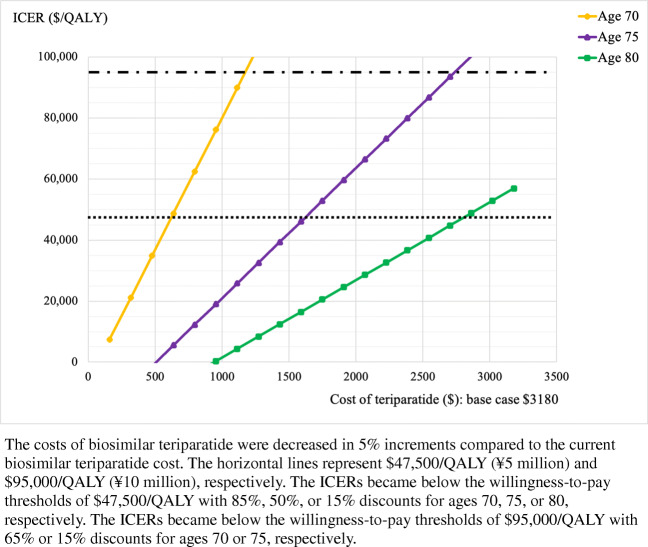
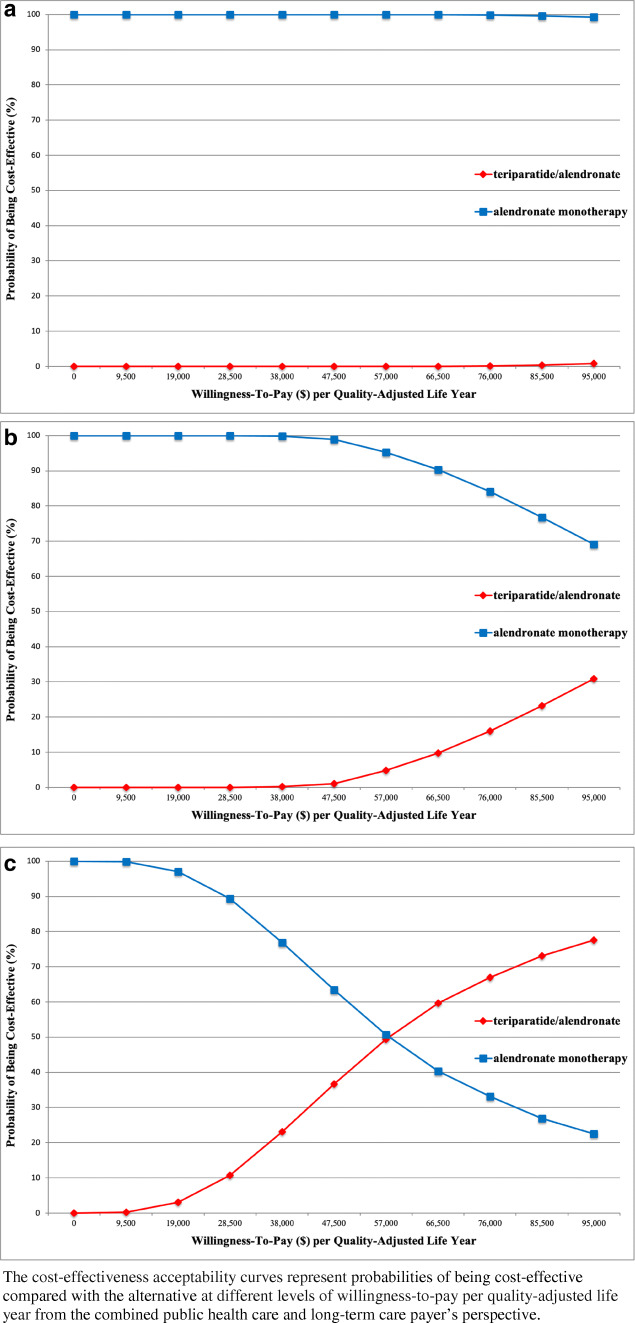
Results: In the base case, sequential teriparatide/alendronate was not cost-effective compared with alendronate monotherapy. In deterministic sensitivity analyses, sequential teriparatide/alendronate would become cost-effective with 85%, 50%, and 15% price discounts to teriparatide at ages 70, 75, and 80, respectively, compared to the current biosimilar cost. Otherwise, results were especially sensitive to changes that affected efficacy of teriparatide or alendronate. In probabilistic sensitivity analyses, the probabilities of sequential teriparatide/alendronate being cost-effective were 0%, 1%, and 37% at ages 70, 75, and 80, respectively.
Conclusions: Among high-risk osteoporotic women in Japan, sequential teriparatide/alendronate was not cost-effective compared with alendronate monotherapy, even with the availability of biosimilar teriparatide.
Keywords: Biosimilar; Cost-effectiveness analysis; Fracture prevention; Osteoporosis; Teriparatide.
Conflict of interest statement
Takahiro Mori: The joint appointment as an associate professor at the University of Tsukuba was sponsored by SMS CO., LTD. in the 2018 financial year (i.e., April 2019 to March 2020), and by FAST DOCTOR CO., LTD in the 2020 financial year (i.e., April 2020 to the present). Neither SMS CO., LTD nor FAST DOCTOR CO., LTD played any role in the conduct of this study.
Carolyn J. Crandall, Tomoko Fujii, and David A. Ganz declare that they have no conflict of interest.
Figures
Similar articles
-
Cost-effectiveness of zoledronic acid compared with sequential denosumab/alendronate for older osteoporotic women in Japan.Arch Osteoporos. 2021 Jul 15;16(1):113. doi: 10.1007/s11657-021-00956-z. Arch Osteoporos. 2021. PMID: 34264429 Free PMC article.
-
Cost-Effectiveness of Sequential Teriparatide/Alendronate Versus Alendronate-Alone Strategies in High-Risk Osteoporotic Women in the US: Analyzing the Impact of Generic/Biosimilar Teriparatide.JBMR Plus. 2019 Nov 13;3(11):e10233. doi: 10.1002/jbm4.10233. eCollection 2019 Nov. JBMR Plus. 2019. PMID: 31768491 Free PMC article.
-
Cost-effectiveness of denosumab versus oral alendronate for elderly osteoporotic women in Japan.Osteoporos Int. 2017 May;28(5):1733-1744. doi: 10.1007/s00198-017-3940-4. Epub 2017 Feb 17. Osteoporos Int. 2017. PMID: 28210776
-
CLINICAL EVALUATION OF COST EFFICACY OF DRUGS FOR TREATMENT OF OSTEOPOROSIS: A META-ANALYSIS.Endocr Pract. 2017 Jul;23(7):841-856. doi: 10.4158/EP161678.RA. Epub 2017 Apr 27. Endocr Pract. 2017. PMID: 28448754 Review.
-
The cost effectiveness of bisphosphonates for the prevention and treatment of osteoporosis: a structured review of the literature.Pharmacoeconomics. 2007;25(11):913-33. doi: 10.2165/00019053-200725110-00003. Pharmacoeconomics. 2007. PMID: 17960951 Review.
Cited by
-
Cost-Effectiveness of Sequential Teriparatide/Zoledronic Acid Compared With Zoledronic Acid Monotherapy for Postmenopausal Osteoporotic Women in China.Front Public Health. 2022 Feb 24;10:794861. doi: 10.3389/fpubh.2022.794861. eCollection 2022. Front Public Health. 2022. PMID: 35284380 Free PMC article.
-
Medical expenditures for fragility hip fracture in Japan: a study using the nationwide health insurance claims database.Arch Osteoporos. 2022 Apr 11;17(1):61. doi: 10.1007/s11657-022-01096-8. Arch Osteoporos. 2022. PMID: 35403938 Free PMC article.
-
Cost-Effectiveness of Sequential Denosumab/Zoledronic Acid Compared With Zoledronic Acid Monotherapy for Postmenopausal Osteoporotic Women in China.Front Pharmacol. 2022 Mar 18;13:816248. doi: 10.3389/fphar.2022.816248. eCollection 2022. Front Pharmacol. 2022. PMID: 35370751 Free PMC article.
-
Management of patients at very high risk of osteoporotic fractures through sequential treatments.Aging Clin Exp Res. 2022 Apr;34(4):695-714. doi: 10.1007/s40520-022-02100-4. Epub 2022 Mar 24. Aging Clin Exp Res. 2022. PMID: 35332506 Free PMC article. Review.
-
The cost-effectiveness of a co-managed care model for elderly hip fracture patients in China: a modelling study.Lancet Reg Health West Pac. 2024 Jul 22;49:101149. doi: 10.1016/j.lanwpc.2024.101149. eCollection 2024 Aug. Lancet Reg Health West Pac. 2024. PMID: 39135908 Free PMC article.
References
-
- Orimo H (ed) (2015, Japanese) Japanese guidelines for prevention and treatment of osteoporosis. Life Science, Tokyo, Japan
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
