

SARS-CoV-2 Cardiac Involvement in Young Competitive Athletes
- PMID: 33866822
- PMCID: PMC8300154
- DOI: 10.1161/CIRCULATIONAHA.121.054824
SARS-CoV-2 Cardiac Involvement in Young Competitive Athletes
Abstract
Background: Cardiac involvement among hospitalized patients with severe coronavirus disease 2019 (COVID-19) is common and associated with adverse outcomes. This study aimed to determine the prevalence and clinical implications of COVID-19 cardiac involvement in young competitive athletes.
Methods: In this prospective, multicenter, observational cohort study with data from 42 colleges and universities, we assessed the prevalence, clinical characteristics, and outcomes of COVID-19 cardiac involvement among collegiate athletes in the United States. Data were collected from September 1, 2020, to December 31, 2020. The primary outcome was the prevalence of definite, probable, or possible COVID-19 cardiac involvement based on imaging definitions adapted from the Updated Lake Louise Imaging Criteria. Secondary outcomes included the diagnostic yield of cardiac testing, predictors for cardiac involvement, and adverse cardiovascular events or hospitalizations.
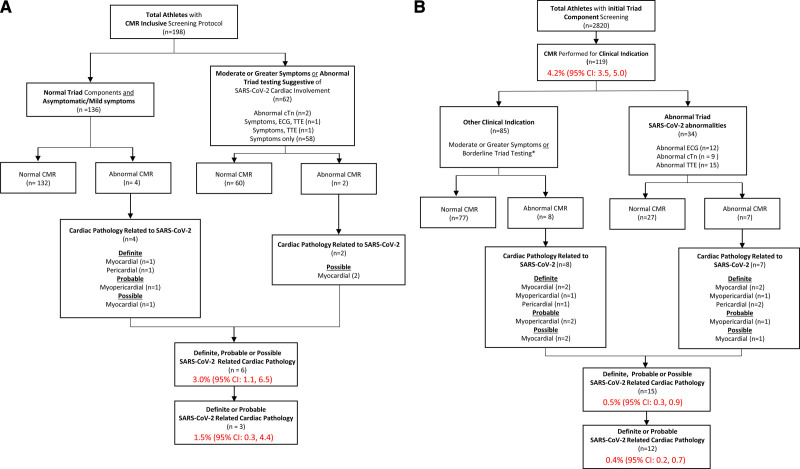
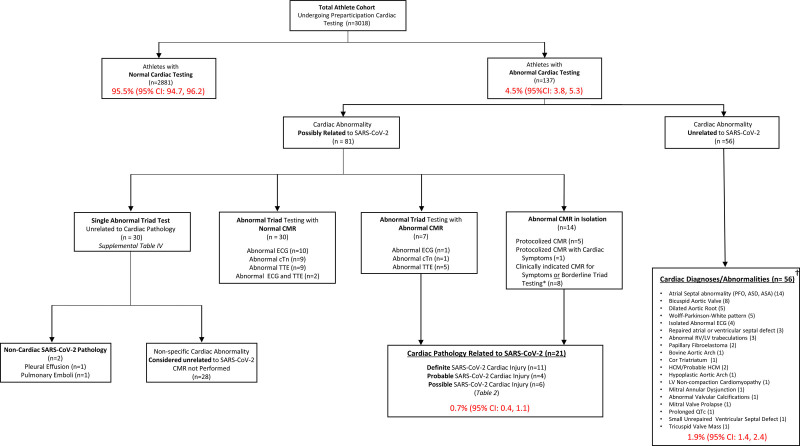
Results: Among 19 378 athletes tested for severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection, 3018 (mean age, 20 years [SD, 1 year]; 32% female) tested positive and underwent cardiac evaluation. A total of 2820 athletes underwent at least 1 element of cardiac triad testing (12-lead ECG, troponin, transthoracic echocardiography) followed by cardiac magnetic resonance imaging (CMR) if clinically indicated. In contrast, primary screening CMR was performed in 198 athletes. Abnormal findings suggestive of SARS-CoV-2 cardiac involvement were detected by ECG (21 of 2999 [0.7%]), cardiac troponin (24 of 2719 [0.9%]), and transthoracic echocardiography (24 of 2556 [0.9%]). Definite, probable, or possible SARS-CoV-2 cardiac involvement was identified in 21 of 3018 (0.7%) athletes, including 15 of 2820 (0.5%) who underwent clinically indicated CMR (n=119) and 6 of 198 (3.0%) who underwent primary screening CMR. Accordingly, the diagnostic yield of CMR for SARS-CoV-2 cardiac involvement was 4.2 times higher for a clinically indicated CMR (15 of 119 [12.6%]) versus a primary screening CMR (6 of 198 [3.0%]). After adjustment for race and sex, predictors of SARS-CoV-2 cardiac involvement included cardiopulmonary symptoms (odds ratio, 3.1 [95% CI, 1.2, 7.7]) or at least 1 abnormal triad test result (odds ratio, 37.4 [95% CI, 13.3, 105.3]). Five (0.2%) athletes required hospitalization for noncardiac complications of COVID-19. During clinical surveillance (median follow-up, 113 days [interquartile range=90 146]), there was 1 (0.03%) adverse cardiac event, likely unrelated to SARS-CoV-2 infection.
Conclusions: SARS-CoV-2 infection among young competitive athletes is associated with a low prevalence of cardiac involvement and a low risk of clinical events in short-term follow-up.
Keywords: COVID-19; SARS-CoV-2; athletes; myocarditis; return to sport.
Figures
Comment in
-
Cardiac Involvement in Athletes Recovering From COVID-19: A Reason for Hope.Circulation. 2021 Jul 27;144(4):267-270. doi: 10.1161/CIRCULATIONAHA.121.054957. Epub 2021 May 18. Circulation. 2021. PMID: 34002620 Free PMC article. No abstract available.
References
-
- Clerkin KJ, Fried JA, Raikhelkar J, Sayer G, Griffin JM, Masoumi A, Jain SS, Burkhoff D, Kumaraiah D, Rabbani L, et al. COVID-19 and cardiovascular disease. Circulation. 2020; 141:1648–1655. doi: 10.1161/CIRCULATIONAHA.120.046941 - PubMed
-
- Eckart RE, Scoville SL, Campbell CL, Shry EA, Stajduhar KC, Potter RN, Pearse LA, Virmani R. Sudden death in young adults: a 25-year review of autopsies in military recruits. Ann Intern Med. 2004; 141:829–834. doi: 10.7326/0003-4819-141-11-200412070-00005 - PubMed
-
- Harmon KG, Asif IM, Maleszewski JJ, Owens DS, Prutkin JM, Salerno JC, Zigman ML, Ellenbogen R, Rao AL, Ackerman MJ, et al. Incidence, cause, and comparative frequency of sudden cardiac death in national collegiate athletic association athletes: a decade in review. Circulation. 2015; 132:10–19. doi: 10.1161/CIRCULATIONAHA.115.015431 - PMC - PubMed
-
- Peterson DF, Kucera K, Thomas LC, Maleszewski J, Siebert D, Lopez-Anderson M, Zigman M, Schattenkerk J, Harmon KG, Drezner JA. Aetiology and incidence of sudden cardiac arrest and death in young competitive athletes in the USA: a 4-year prospective study [published online March 30, 2020]. Br J Sports Med. doi: 10.1136/bjsports-2020-102666. https://bjsm.bmj.com/content/early/2021/05/09/bjsports-2020-102666.info - PMC - PubMed
-
- American Medical Society for Sports Medicine and the American College of Cardiology. Cardiac Considerations for College Student-Athletes During the COVID-19 Pandemic. Published 2020. https://www.amssm.org/Content/pdf-files/COVID19/NCAA-COVID19/NCAA-COVID-...
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
