

Detection of Domestic Violence and Abuse by Community Mental Health Teams Using the BRAVE Intervention: A Multicenter, Cluster Randomized Controlled Trial
- PMID: 33866860
- PMCID: PMC9382347
- DOI: 10.1177/08862605211004177
Detection of Domestic Violence and Abuse by Community Mental Health Teams Using the BRAVE Intervention: A Multicenter, Cluster Randomized Controlled Trial
Abstract
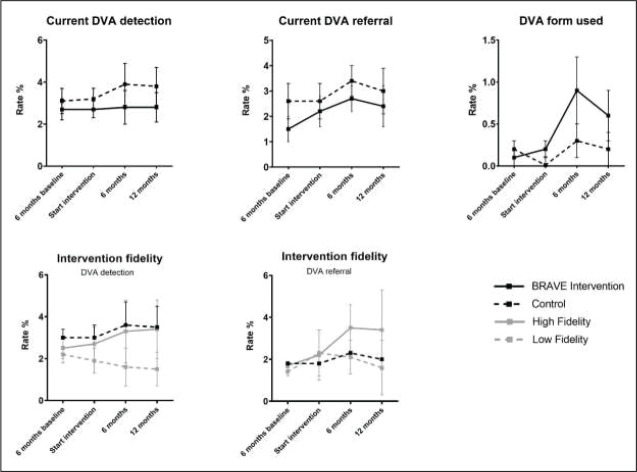
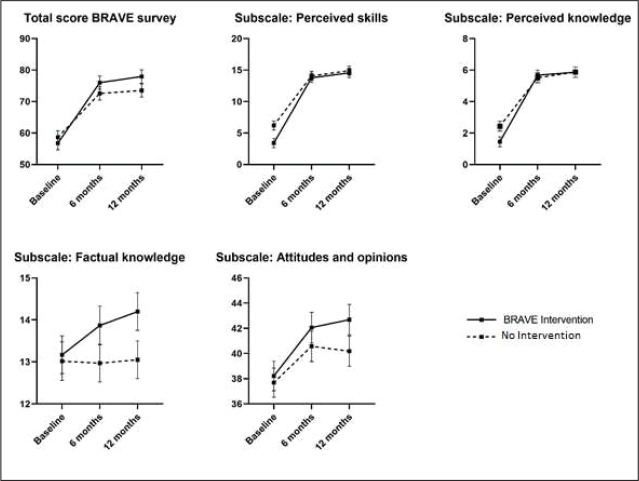
Despite increased prevalence of domestic violence and abuse (DVA), victimization through DVA often remains undetected in mental health care. To estimate the effectiveness of a system provider level training intervention by comparing the detection and referral rates of DVA of intervention community mental health (CMH) teams with rates in control CMH teams. We also aimed to determine whether improvements in knowledge, skills and attitudes to DVA were greater in clinicians working in intervention CMH teams than those working in control teams. We conducted a cluster randomized controlled trial in two urban areas of the Netherlands. Detection and referral rates were assessed at baseline and at 6 and 12 months after the start of the intervention. DVA knowledge, skills and attitudes were assessed using a survey at baseline and at 6 and 12 months after start of the intervention. Electronic patient files were used to identify detected and referred cases of DVA. Outcomes were compared between the intervention and control teams using a generalized linear mixed model. During the 12-month follow-up, detection and referral rates did not differ between the intervention and control teams. However, improvements in knowledge, skills and attitude during that follow-up period were greater in intervention teams than in control teams: β 3.21 (95% CI 1.18-4.60). Our trial showed that a training program on DVA knowledge and skills in CMH teams can increase knowledge and attitude towards DVA. However, our intervention does not appear to increase the detection or referral rates of DVA in patients with a severe mental illness. A low detection rate of DVA remains a major problem. Interventions with more obligatory elements and a focus on improving communication between CMH teams and DVA services are recommended.
Keywords: domestic violence and abuse; interpersonal violence; outreaching healthcare; randomized controlled trial; severe mental illness; victimization.
Conflict of interest statement
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Figures
References
-
- Arkins B., Begley C., & Higgins A. (2016). Measures for screening for intimate partner violence: A systematic review. Journal of Psychiatric and Mental Health Nursing, 23(3-4), 217-235. https://doi.org/10.1111/jpm.12289 - PubMed
-
- Beyer F., Sidarus N., Bonicalzi S., & Haggard P. (2017). Beyond self-serving bias: Diffusion of responsibility reduces sense of agency and outcome monitoring. Social Cognitive and Affective Neuroscience, 12(1), 138-145. https://doi.org/10.1093/scan/nsw160 - PMC - PubMed
-
- Campbell J. C. (2002). Health consequences of intimate partner violence. Lancet, 359(9314), 1331-1336. - PubMed
-
- Campbell M. K., Piaggio G., Elbourne D. R., Altman D. G., & Group C. (2012). Consort 2010 statement: Extension to cluster randomised trials. BMJ, 345, Article e5661. https://doi.org/10.1136/bmj.e5661 - PubMed
-
- Carmo R. A., Melo A. P. S., Dezanet L. N. C., De Oliveira H. N., Cournos F., & Guimaraes M. D. C. (2014). Correlates of hepatitis b among patients with mental illness in Brazil. General Hospital Psychiatry, 36(4), 398-405. https://doi.org/10.1016/j.genhosppsych.2014.03.001 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
