

Changes in Magnetic Resonance Imaging Using the Prostate Cancer Radiologic Estimation of Change in Sequential Evaluation Criteria to Detect Prostate Cancer Progression for Men on Active Surveillance
- PMID: 33867045
- PMCID: PMC9310665
- DOI: 10.1016/j.euo.2020.09.004
Changes in Magnetic Resonance Imaging Using the Prostate Cancer Radiologic Estimation of Change in Sequential Evaluation Criteria to Detect Prostate Cancer Progression for Men on Active Surveillance
Abstract
Background: The ability of serial magnetic resonance imaging (MRI) to capture pathologic progression during active surveillance (AS) remains in question.
Objective: To determine whether changes in MRI are associated with pathologic progression for patients on AS.
Design, setting, and participants: From July 2007 through January 2020, we identified all patients evaluated for AS at our institution. Following confirmatory biopsy, a total of 391 patients who underwent surveillance MRI and biopsy at least once were identified (median follow-up of 35.6 mo, interquartile range 19.7-60.6).
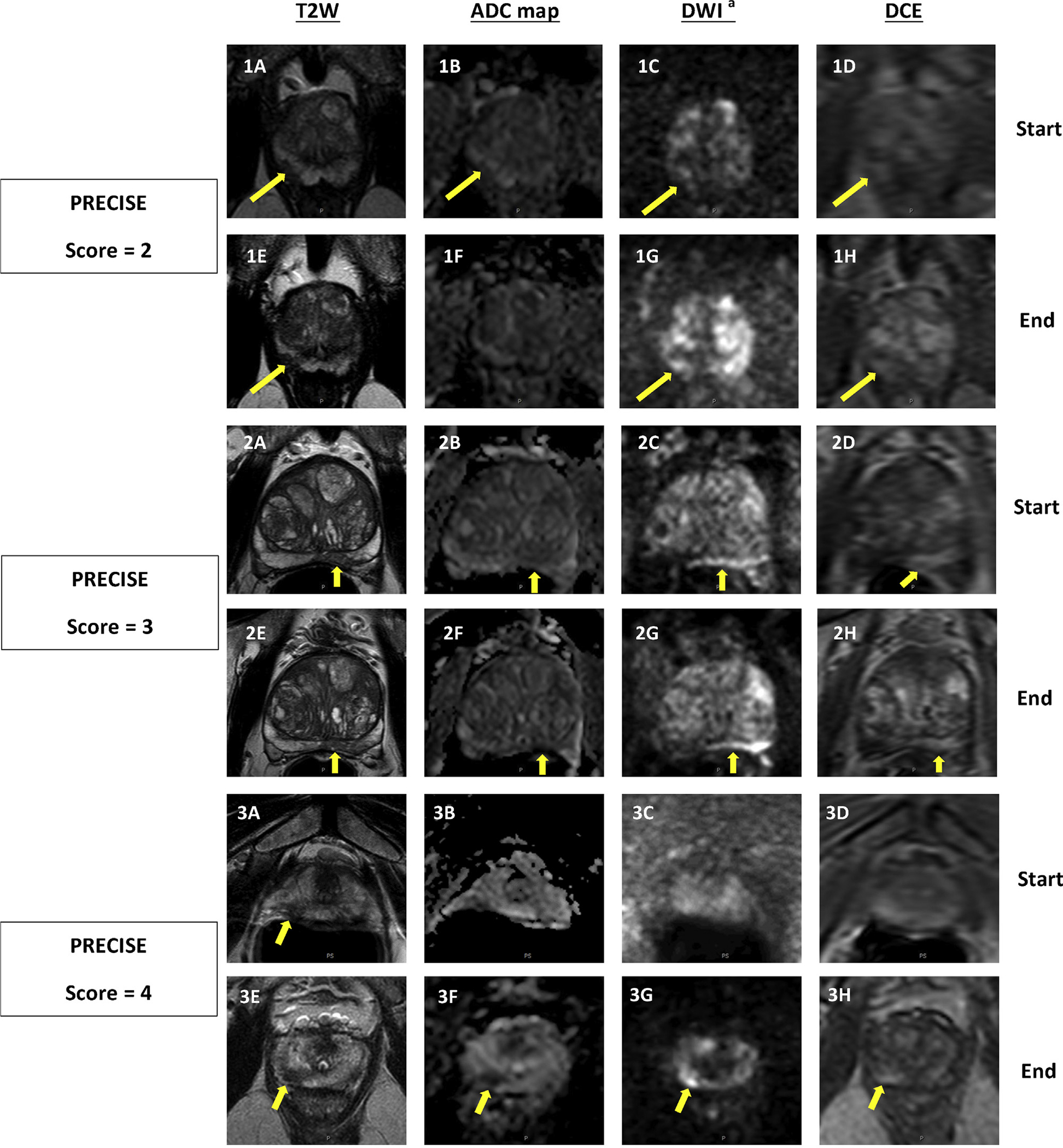
Outcome measurements and statistical analysis: All MRI intervals were scored using the "Prostate Cancer Radiologic Estimation of Change in Sequential Evaluation" (PRECISE) criteria, with PRECISE scores =4 considered a positive change in MRI. A generalized estimating equation-based logistic regression analysis was conducted for all intervals with a PRECISE score of <4 to determine the predictors of Gleason grade group (GG) progression despite stable MRI.
Results and limitations: A total of 621 MRI intervals were scored by PRECISE and validated by biopsy. The negative predictive value of stable MRI (PRECISE score <4) was greatest for detecting GG1 to?=?GG3 disease (0.94 [0.91-0.97]). If 2-yr surveillance biopsy were performed exclusively for a positive change in MRI, 3.7% (4/109) of avoided biopsies would have resulted in missed progression from GG1 to?=?GG3 disease. Prostate-specific antigen (PSA) density (odds ratio 1.95 [1.17-3.25], p?=? 0.01) was a risk factor for progression from GG1 to =GG3 disease despite stable MRI.
Conclusions: In patients with GG1 disease and stable MRI (PRECISE score <4) on surveillance, grade progression to?=?GG3 disease is not common. In patients with grade progression detected on biopsy despite stable MRI, elevated PSA density appeared to be a risk factor for progression to?=?GG3 disease.
Patient summary: For patients with low-risk prostate cancer on active surveillance, the risk of progressing to grade group 3 disease is low with a stable magnetic resonance image (MRI) after 2?yr. Having higher prostate-specific antigen density increases the risk of progression, despite having a stable MRI.
Keywords: Active surveillance; Fusion biopsy; Multiparametric magnetic resonance imaging; Prostate Cancer Radiologic Estimation of Change in Sequential Evaluation; Prostate cancer.
Copyright © 2020. Published by Elsevier B.V.
Conflict of interest statement
Figures
Comment in
-
Let's Follow the Golden Mean: Using Magnetic Resonance Imaging to Determine the Need for Biopsy in Men on Active Surveillance.Eur Urol Oncol. 2021 Apr;4(2):235-236. doi: 10.1016/j.euo.2020.11.009. Epub 2020 Dec 23. Eur Urol Oncol. 2021. PMID: 33358393 No abstract available.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
