

Risk of Symptomatic Kidney Stones During and After Pregnancy
- PMID: 33867205
- PMCID: PMC8384636
- DOI: 10.1053/j.ajkd.2021.01.008
Risk of Symptomatic Kidney Stones During and After Pregnancy
Abstract
Rationale & objective: There are several well-known anatomical and physiological changes during pregnancy that could contribute to kidney stone formation, but evidence that they increase the risk of kidney stones during pregnancy is lacking. We determined whether there was an increased risk of a first-time symptomatic kidney stone during and after pregnancy.
Study design: A population-based matched case-control study.
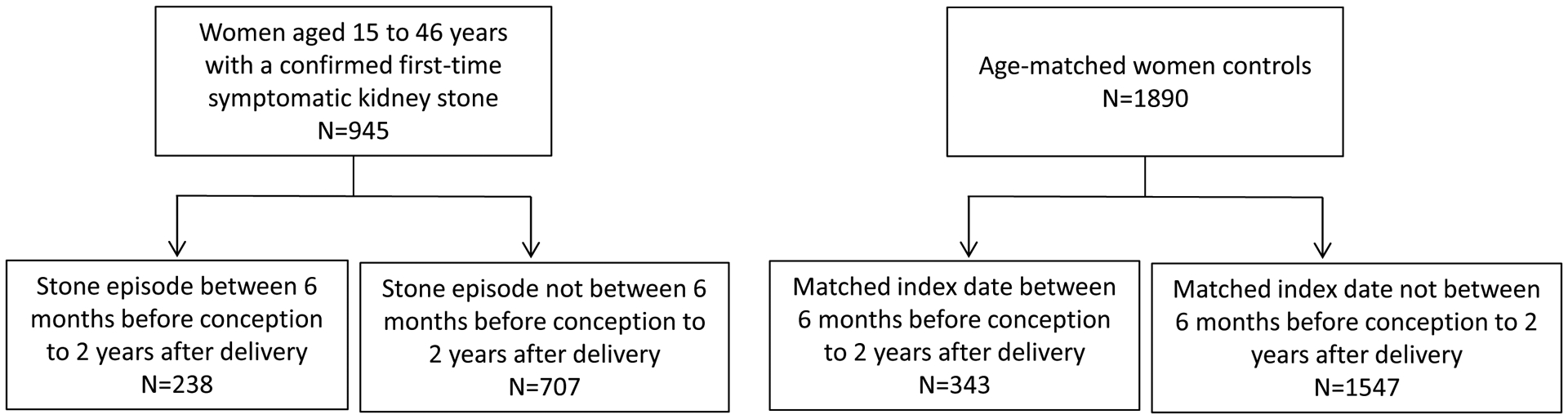
Setting & participants: 945 female first-time symptomatic kidney stone formers aged 15-45 years and 1,890 age-matched female controls in Olmsted County, MN, from 1984-2012. The index date was the date of onset of a symptomatic kidney stone for both the case and her matched controls.
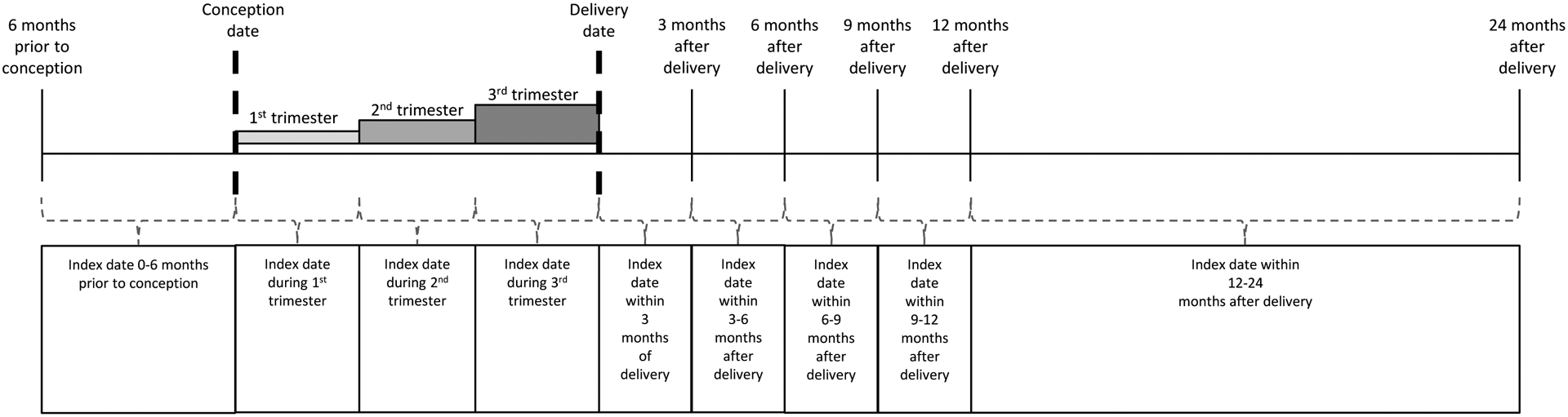
Exposure: The primary exposure was pregnancy with assessment for variation in risk across different time intervals before, during, and after pregnancy. Medical records were manually reviewed to determine the conception and delivery dates for pregnancies.
Outcome: Medical record-validated first-time symptomatic kidney stone.
Analytical approach: Conditional and unconditional multivariable logistic regression analysis.
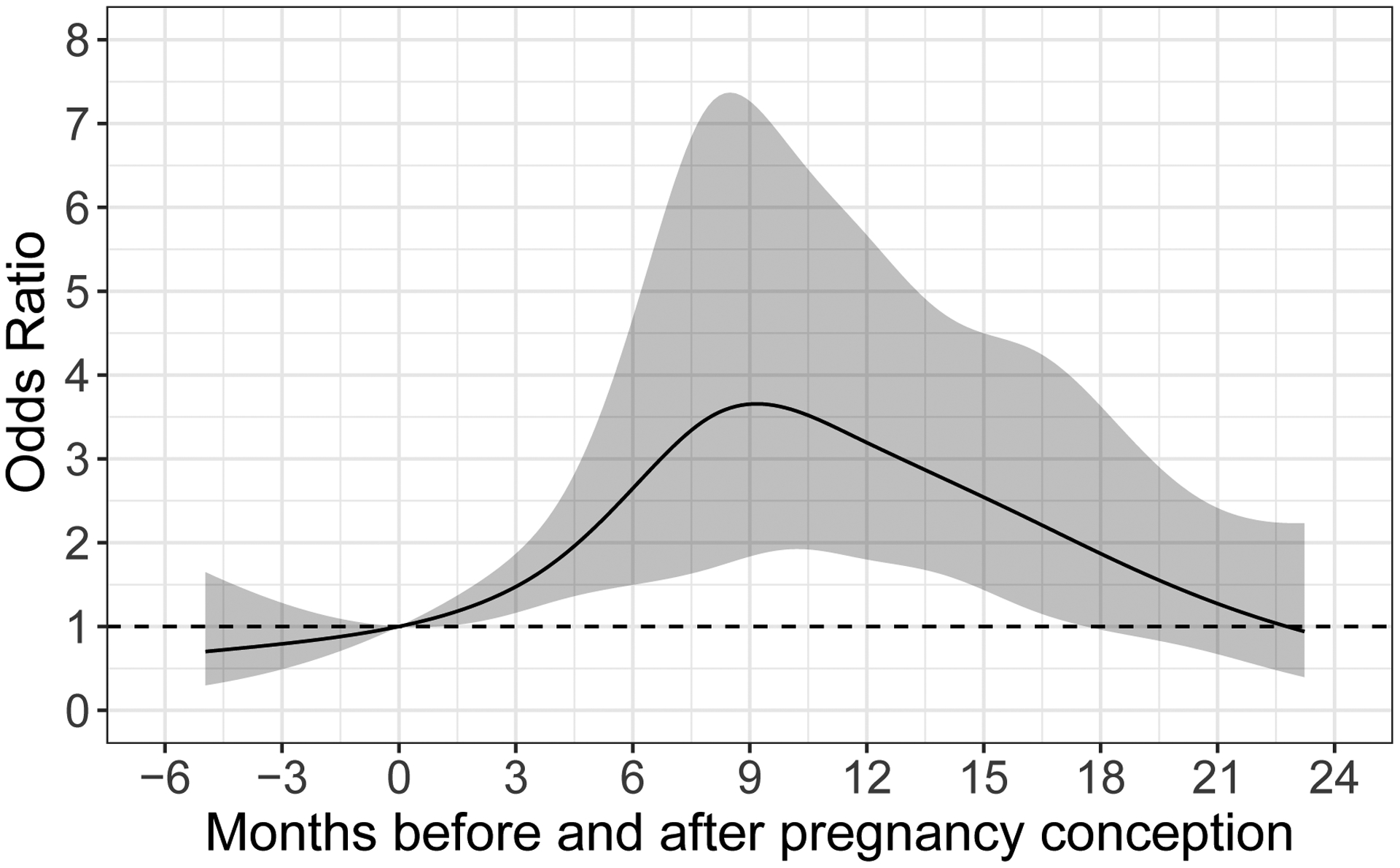
Results: Compared with nonpregnant women, the odds of a symptomatic kidney stone forming in women was similar in the first trimester (OR, 0.92; P=0.8), began to increase during the second trimester (OR, 2.00; P=0.007), further increased during the third trimester (OR, 2.69; P=0.001), peaked at 0 to 3 months after delivery (OR, 3.53; P<0.001), and returned to baseline by 1year after delivery. These associations persisted after adjustment for age and race or for diabetes mellitus, hypertension, and obesity. These results did not significantly differ by age, race, time period, or number of prior pregnancies. Having a prior pregnancy (delivery date>1year ago) was also associated with a first-time symptomatic kidney stone (OR, 1.27; P=0.01).
Limitations: Observational study design in a predominantly White population. The exact timing of stone formation cannot be determined.
Conclusions: Pregnancy increases the risk of a first-time symptomatic kidney stone. This risk peaks close to delivery and then improves by 1 year after delivery, though a modest risk of a kidney stone still exists beyond 1 year after delivery.
Keywords: Computed tomography (CT); hydronephrosis; imaging; kidney stones; nephrolithiasis; obstetric complications; population-based; pregnancy; recurrence; stone composition; symptoms; ultrasound.
Copyright © 2021 National Kidney Foundation, Inc. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Urolithiasis/Endourology.J Urol. 2021 Dec;206(6):1513-1515. doi: 10.1097/JU.0000000000002207. Epub 2021 Sep 8. J Urol. 2021. PMID: 34494454 No abstract available.
References
-
- Semins MJ, Matlaga BR. Kidney stones during pregnancy. Nat Rev Urol. 2014;11(3): 163–168. - PubMed
-
- Riley JM, Dudley AG, Semins MJ. Nephrolithiasis and pregnancy: has the incidence been rising? J Endourol. 2014;28(3): 383–386. - PubMed
-
- Ordon M, Dirk J, Slater J, Kroft J, Dixon S, Welk B. Incidence, Treatment, and Implications of Kidney Stones During Pregnancy: A Matched Population-Based Cohort Study. J Endourol 2020;34(2): 215–221. - PubMed
-
- Rosenberg E, Sergienko R, Abu-Ghanem S, et al.Nephrolithiasis during pregnancy: characteristics, complications, and pregnancy outcome. World J Urol. 2011;29(6): 743–747. - PubMed
-
- Swartz MA, Lydon-Rochelle MT, Simon D, Wright JL, Porter MP. Admission for nephrolithiasis in pregnancy and risk of adverse birth outcomes. Obstet Gynecol. 2007;109(5): 1099–1104. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
