

The Placebo and Nocebo Responses in Clinical Trials in Inflammatory Bowel Diseases
- PMID: 33867990
- PMCID: PMC8044413
- DOI: 10.3389/fphar.2021.641436
The Placebo and Nocebo Responses in Clinical Trials in Inflammatory Bowel Diseases
Abstract
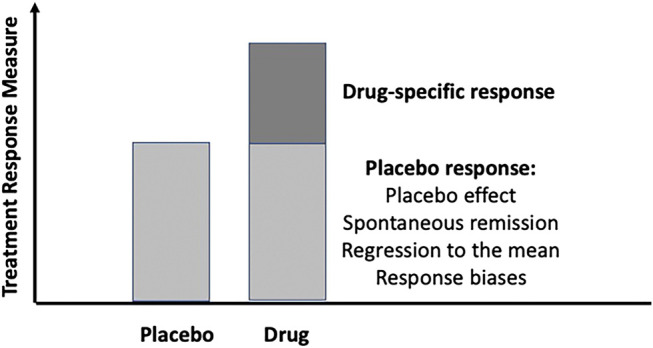
Placebo and nocebo responses are mostly discussed in clinical trials with functional bowel disorders. Much less has been investigated and is known in gastrointestinal diseases beyond irritable bowel syndrome (IBS), especially in inflammatory bowel diseases (IBD). For the purpose of this review, we screened the Journal of Interdisciplinary Placebo Studies (JIPS) database with approximately 4,500 genuine placebo research articles and identified nine meta-analyses covering more than 135 randomized and placebo-controlled trials (RCTs) with more than 10,000 patients with Crohn´s disease (CD) and another five meta-analyses with 150 RCTs and more than 10,000 patients with ulcerative colitis (UC). Only three discussed nocebo effects, especially in the context of clinical use of biosimilars to treat inflammation. The articles were critically analyzed with respect to the size of the placebo response in CD and UC, its effects on clinical improvement versus maintenance of remission, and mediators and moderators of the response identified. Finally, we discussed and compared the differences and similarities of the placebo responses in IBD and IBS and the nocebo effect in switching from biologics to biosimilars in IBD management.
Keywords: Crohn´s disease; clinical trial; inflammatory bowel disease; placebo and nocebo effects; systematic (literature) review; ulcerative colitis.
Copyright © 2021 Enck and Klosterhalfen.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Biesiekierski J. R., Peters S. L., Newnham E. D., Rosella O., Muir J. G., Gibson P. R. (2013). No effects of gluten in patients with self-reported non-celiac gluten sensitivity after dietary reduction of fermentable, poorly absorbed, short-chain carbohydrates. Gastroenterology 145 (2), 320. 10.1053/j.gastro.2013.04.051 - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources