

Bone defect reconstruction via endochondral ossification: A developmental engineering strategy
- PMID: 33868628
- PMCID: PMC8020769
- DOI: 10.1177/20417314211004211
Bone defect reconstruction via endochondral ossification: A developmental engineering strategy
Abstract
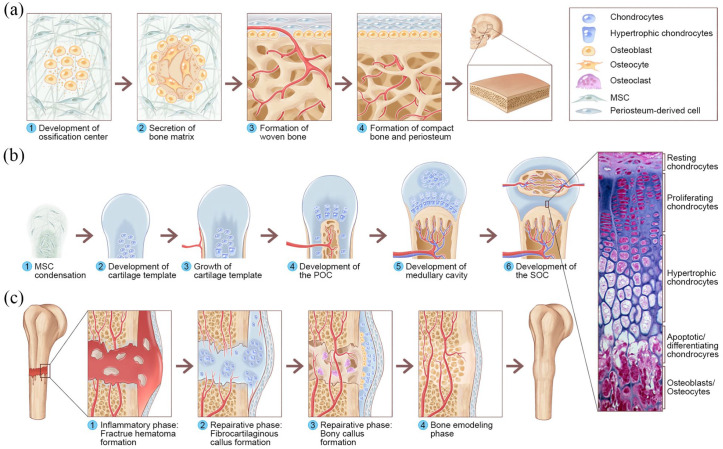
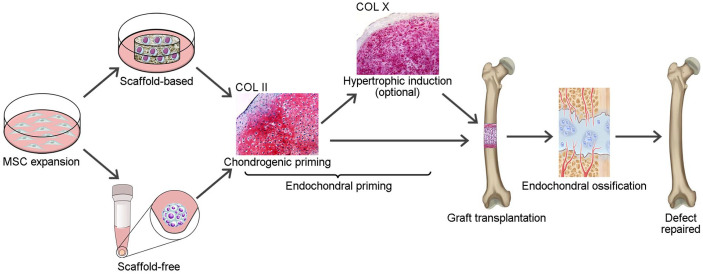
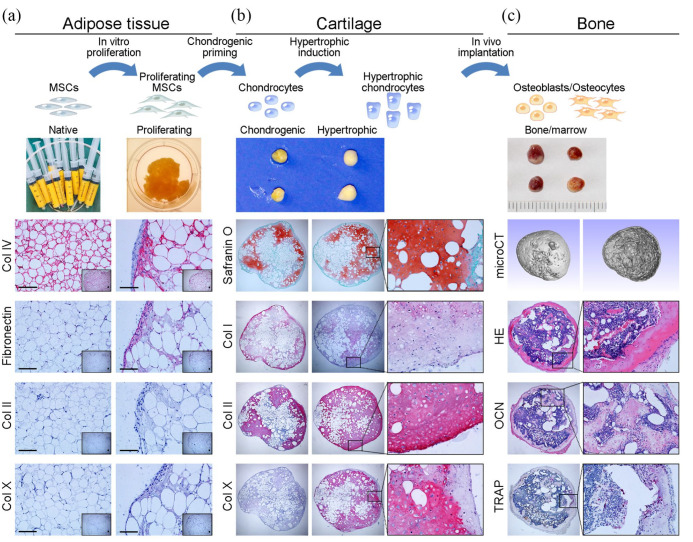
Traditional bone tissue engineering (BTE) strategies induce direct bone-like matrix formation by mimicking the embryological process of intramembranous ossification. However, the clinical translation of these clinical strategies for bone repair is hampered by limited vascularization and poor bone regeneration after implantation in vivo. An alternative strategy for overcoming these drawbacks is engineering cartilaginous constructs by recapitulating the embryonic processes of endochondral ossification (ECO); these constructs have shown a unique ability to survive under hypoxic conditions as well as induce neovascularization and ossification. Such developmentally engineered constructs can act as transient biomimetic templates to facilitate bone regeneration in critical-sized defects. This review introduces the concept and mechanism of developmental BTE, explores the routes of endochondral bone graft engineering, highlights the current state of the art in large bone defect reconstruction via ECO-based strategies, and offers perspectives on the challenges and future directions of translating current knowledge from the bench to the bedside.
Keywords: Developmental engineering; bone defect reconstruction; bone tissue engineering; endochondral ossification; hypertrophic cartilage.
© The Author(s) 2021.
Conflict of interest statement
Declaration of conflicting interests: The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
References
-
- Buser Z, Brodke DS, Youssef JA, et al. Synthetic bone graft versus autograft or allograft for spinal fusion: a systematic review. J Neurosurg Spine 2016; 25: 509–516. - PubMed
-
- Roseti L, Parisi V, Petretta M, et al. Scaffolds for bone tissue engineering: state of the art and new perspectives. Mater Sci Eng C Mater Biol Appl 2017; 78: 1246–1262. - PubMed
-
- Wubneh A, Tsekoura EK, Ayranci C, et al. Current state of fabrication technologies and materials for bone tissue engineering. Acta Biomater 2018; 80: 1–30. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
