

Use of a Smartphone to Gather Parkinson's Disease Neurological Vital Signs during the COVID-19 Pandemic
- PMID: 33868630
- PMCID: PMC8035908
- DOI: 10.1155/2021/5534282
Use of a Smartphone to Gather Parkinson's Disease Neurological Vital Signs during the COVID-19 Pandemic
Abstract
Introduction: To overcome travel restrictions during the COVID-19 pandemic, consumer-based technology was rapidly deployed to the smartphones of individuals with Parkinson's disease (PD) participating in a 12-month exercise trial. The aim of the project was to determine the feasibility of utilizing a combined synchronous and asynchronous self-administered smartphone application to characterize PD symptoms.
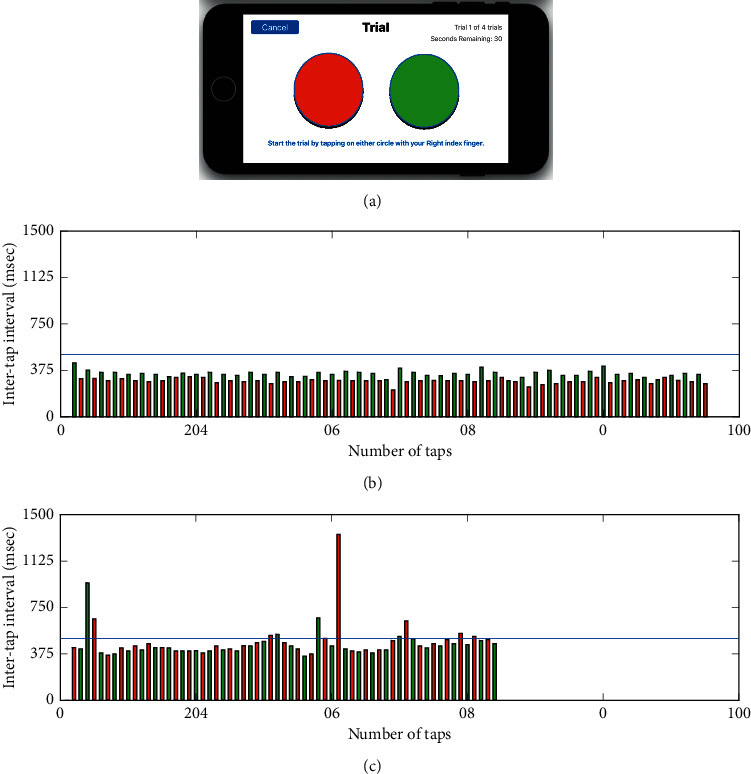
Methods: A synchronous video virtual visit was completed for the administration of virtual Movement Disorder Society-Unified Parkinson's Disease Rating Scale III (vMDS-UPDRS III). Participants asynchronously completed a mobile application consisting of a measure of upper extremity bradykinesia (Finger Tapping Test) and information processing.
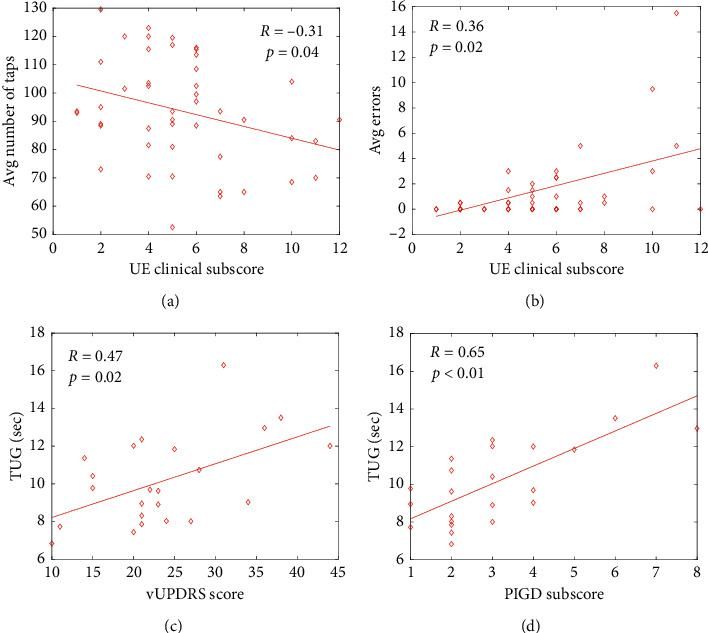
Results: Twenty-three individuals completed the assessments. The mean vMDS-UPDRS III was 23.65 ± 8.56 points. On average, the number of taps was significantly greater for the less affected limb, 97.96 ± 17.77 taps, compared to the more affected, 89.33 ± 18.66 taps (p = 0.025) with a significantly greater number of freezing episodes for the more affected limb (p < 0.05). Correlation analyses indicated the number of errors and the number of freezing episodes were significantly related to clinical ratings of vMDS-UPDRS III bradykinesia (Rho = 0.44, p < 0.01; R = 0.43, p < 0.01, resp.) and finger tapping performance (Rho = 0.31, p = 0.03; Rho = 0.32, p = 0.03, resp.). Discussion. The objective characterization of bradykinesia, akinesia, and nonmotor function and their relationship with clinical disease metrics indicate smartphone technology provides a remote method of characterizing important aspects of PD performance. While theoretical and position papers have been published on the potential of telemedicine to aid in the management of PD, this report translates the theory into a viable reality.
Copyright © 2021 Jay L. Alberts et al.
Conflict of interest statement
The authors have no financial disclosures to declare related to this article.
Figures
References
-
- World Health Organization. Telemedicine: Opportunities and Developments in Member States: Report on the Second Global Survey on eHealth 2009. Geneva, Switzerland: World Health Organization; 2010. https://www.who.int/goe/publications/goe_telemedicine_2010.pdf.
LinkOut - more resources
Full Text Sources
Other Literature Sources
