

"Trap Door" Orbital Floor Fractures in Adults: Are They Different from Pediatric Fractures?
- PMID: 33868879
- PMCID: PMC8049158
- DOI: 10.1097/GOX.0000000000003537
"Trap Door" Orbital Floor Fractures in Adults: Are They Different from Pediatric Fractures?
Abstract
Background: "Trap door" orbital floor fractures are usually seen in children. In the linear fracture type, a break occurs in the bones of the orbital floor that permits orbital tissue to prolapse into the fracture site during fracture formation. The bony fragments of the fracture then return to their original position, entrapping the prolapsed orbital tissue. In the hinged fracture type, the fractured part of the floor is minimally displaced into the maxillary sinus and acts as the hinge of a "swinging door" entrapping the orbital tissue.
Methods: We report on a series of 10 adult patients with hinged orbital floor fractures.
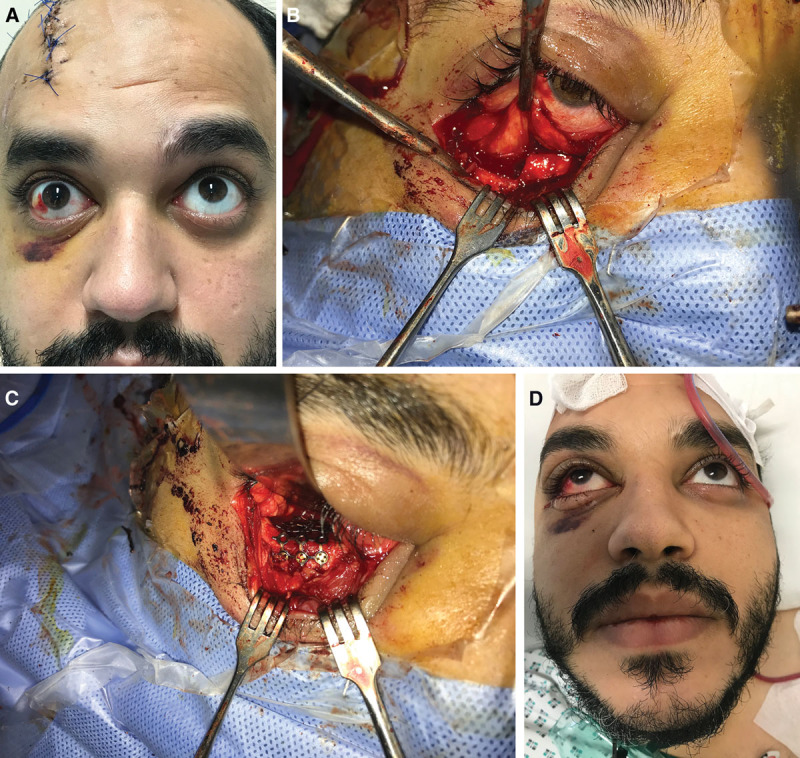
Results: The mean patient age was 35 years. Seven patients had a pure orbital floor fracture and the remaining 3 patients had fractures of both the orbital floor and the inferior orbital rim. All 10 patients had diplopia in the upgaze. None of the patients had signs of the oculocardiac reflex. None of the CT scans showed a "tear-drop" sign. However, the sagittal CT scans showed evidence of entrapment of the inferior rectus. All patients had a small area of a slightly depressed orbital floor at the site of entrapment, without a bony defect. All patients underwent surgery through an infraorbital incision and a titanium mesh was used in all patients. There were no postoperative complications. All patients regained full range of motion of the globe.
Conclusion: This is the first series in the literature that reports on the characteristics and outcome of trap door orbital floor fractures in adults.
Copyright © 2021 The Authors. Published by Wolters Kluwer Health, Inc. on behalf of The American Society of Plastic Surgeons.
Conflict of interest statement
Disclosure: The authors have no financial interest to declare in relation to the content of this article.
Figures





Similar articles
-
Orbital blow-out fractures: correlation of preoperative computed tomography and postoperative ocular motility.Trans Am Ophthalmol Soc. 1998;96:329-47; discussion 347-53. Trans Am Ophthalmol Soc. 1998. PMID: 10360296 Free PMC article.
-
Management of pure orbital floor fractures: a proposed protocol to prevent unnecessary or early surgery.Orbit. 2014 Oct;33(5):336-42. doi: 10.3109/01676830.2014.902475. Epub 2014 Jul 2. Orbit. 2014. PMID: 24987818
-
Pediatric orbital floor trapdoor fractures: outcomes and CT-based morphologic assessment of the inferior rectus muscle.J Plast Reconstr Aesthet Surg. 2012 Jul;65(7):869-74. doi: 10.1016/j.bjps.2012.02.004. Epub 2012 Mar 28. J Plast Reconstr Aesthet Surg. 2012. PMID: 22459795
-
Clinical recommendations for repair of isolated orbital floor fractures: an evidence-based analysis.Ophthalmology. 2002 Jul;109(7):1207-10; discussion 1210-1; quiz 1212-3. doi: 10.1016/s0161-6420(02)01057-6. Ophthalmology. 2002. PMID: 12093637 Review.
-
Non-displaced pediatric orbital fracture with displacement of the inferior rectus muscle into the maxillary sinus: a case report and review of the literature.Int J Oral Maxillofac Surg. 2014 Jan;43(1):29-31. doi: 10.1016/j.ijom.2013.04.021. Epub 2013 Jun 28. Int J Oral Maxillofac Surg. 2014. PMID: 23810679 Review.
Cited by
-
Pediatric orbital fractures in Singapore: demographics, etiology, and the role of bioresorbable implants.Front Ophthalmol (Lausanne). 2025 Mar 13;5:1506445. doi: 10.3389/fopht.2025.1506445. eCollection 2025. Front Ophthalmol (Lausanne). 2025. PMID: 40182536 Free PMC article.
-
Characteristics and surgical management of pure trapdoor fracture of the orbital floor in adults: a 15-year review.Oral Maxillofac Surg. 2023 Dec;27(4):625-630. doi: 10.1007/s10006-022-01099-2. Epub 2022 Jul 16. Oral Maxillofac Surg. 2023. PMID: 35841436 Free PMC article.
-
A Comprehensive Look at Maxillofacial Traumas: On the Basis of Orbital Involvement.Diagnostics (Basel). 2023 Nov 11;13(22):3429. doi: 10.3390/diagnostics13223429. Diagnostics (Basel). 2023. PMID: 37998566 Free PMC article.
-
The Usefulness of the Navigation System to Reconstruct Orbital Wall Fractures Involving Inferomedial Orbital Strut.J Clin Med. 2023 Jul 28;12(15):4968. doi: 10.3390/jcm12154968. J Clin Med. 2023. PMID: 37568370 Free PMC article.
References
-
- Gerbino G, Roccia F, Bianchi FA, et al. . Surgical management of orbital trapdoor fracture in a pediatric population. J Oral Maxillofac Surg. 2010; 68:1310–1316 - PubMed
-
- Silverman N, Spindle J, Tang SX, et al. . Orbital floor fracture with entrapment: Imaging and clinical correlations in 45 cases. Orbit. 2017; 36:331–336 - PubMed
-
- Mehmood N, Hasan A. Oculocardiac reflex: an underrecognized but important association with orbital trap door fractures. Pediatr Emerg Care. [published online ahead of print August 9, 2019] - PubMed
-
- Jordan DR, Allen LH, White J, et al. . Intervention within days for some orbital floor fractures: the white-eyed blowout. Ophthalmic Plast Reconstr Surg. 1998; 14:379–390 - PubMed
-
- McInnes AW, Burnstine MA. White-eyed medial wall orbital blowout fracture. Ophthalmic Plast Reconstr Surg. 2010; 26:44–46 - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources