

Survival Comparisons of Hepatic Arterial Infusion Chemotherapy With mFOLFOX and Transarterial Chemoembolization in Patients With Unresectable Intrahepatic Cholangiocarcinoma
- PMID: 33868997
- PMCID: PMC8047640
- DOI: 10.3389/fonc.2021.611118
Survival Comparisons of Hepatic Arterial Infusion Chemotherapy With mFOLFOX and Transarterial Chemoembolization in Patients With Unresectable Intrahepatic Cholangiocarcinoma
Abstract
Background: Intrahepatic cholangiocarcinoma (ICC) has a poor prognosis and 40%-60% of patients present with advanced disease at the time of diagnosis. Transarterial chemoembolization (TACE) and hepatic arterial infusion chemotherapy (HAIC) have recently been used in unresectable ICC. The aim of this study was to compare the survival differences of unresectable ICC patients after TACE and HAIC treatment.
Methods: Between March 2011 and October 2019, a total of 126 patients with unresectable ICC, as evident from biopsies and imaging, and who had received TACE or HAIC were enrolled in this study. Baseline characteristics and survival differences were compared between the TACE and HAIC treatment groups.
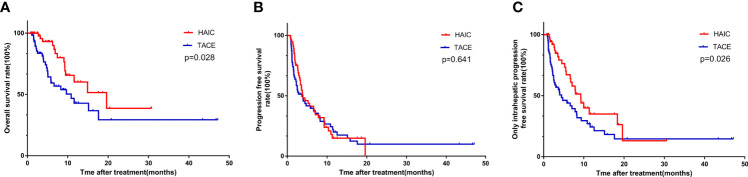
Results: ICC Patients had significantly higher survival rates after the HAIC treatment, compared with those after TACE treatment [1-year overall survival (OS) rates: 60.2% vs. 42.9%, 2-year OS rates: 38.7% vs. 29.4%, P=0.028; 1-year progression-free survival (PFS) rates: 15.0% vs. 20.0%, 2-year PFS rates: 0% vs. 0%, P=0.641; 1-year only intrahepatic PFS (OIPFS) rates: 35.0% vs. 24.4%, 2-year OIPFS rates: 13.1% vs. 14.6%, P = 0.026]. Multivariate Cox regression analysis showed that HAIC was a significant and independent factor for OS and OIPFS in the study cohort.
Conclusions: HAIC is superior to TACE for treatment of unresectable ICC. A new tumor response evaluation procedure for HAIC treatment in unresectable ICC patients is needed to provide better therapeutic strategies. A randomized clinical trial comparing the survival benefits of HAIC and TACE is therefore being considered.
Keywords: hepatic arterial infusion chemotherapy; intrahepatic cholangiocarcinoma; only intrahepatic progression-free survival; overall survival; transarterial chemoembolization.
Copyright © 2021 Cai, He, Zhao and Lin.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

Similar articles
-
Hepatic arterial infusion chemotherapy versus transarterial chemoembolization in patients with unresectable intrahepatic cholangiocarcinoma: a multicenter retrospective cohort study.Eur Radiol. 2025 Apr 11. doi: 10.1007/s00330-025-11557-6. Online ahead of print. Eur Radiol. 2025. PMID: 40216615
-
Hepatic artery infusion chemotherapy using mFOLFOX versus transarterial chemoembolization for massive unresectable hepatocellular carcinoma: a prospective non-randomized study.Chin J Cancer. 2017 Oct 23;36(1):83. doi: 10.1186/s40880-017-0251-2. Chin J Cancer. 2017. PMID: 29061175 Free PMC article. Clinical Trial.
-
Comparative study on the efficacy and safety of transarterial chemoembolization combined with hepatic arterial infusion chemotherapy for large unresectable hepatocellular carcinoma.J Gastrointest Oncol. 2024 Feb 29;15(1):346-355. doi: 10.21037/jgo-23-821. Epub 2024 Feb 28. J Gastrointest Oncol. 2024. PMID: 38482220 Free PMC article.
-
Hepatic arterial infusion chemotherapy versus transarterial chemoembolization for unresectable hepatocellular carcinoma: A systematic review with meta-analysis.Front Bioeng Biotechnol. 2022 Sep 27;10:1010824. doi: 10.3389/fbioe.2022.1010824. eCollection 2022. Front Bioeng Biotechnol. 2022. PMID: 36237208 Free PMC article.
-
HAIC versus TACE for patients with unresectable hepatocellular carcinoma: A systematic review and meta-analysis.Medicine (Baltimore). 2022 Dec 23;101(51):e32390. doi: 10.1097/MD.0000000000032390. Medicine (Baltimore). 2022. PMID: 36595819 Free PMC article.
Cited by
-
Techniques and status of hepatic arterial infusion chemotherapy for primary hepatobiliary cancers.Ther Adv Med Oncol. 2024 Jan 27;16:17588359231225040. doi: 10.1177/17588359231225040. eCollection 2024. Ther Adv Med Oncol. 2024. PMID: 38282664 Free PMC article. Review.
-
Hepatic arterial infusion chemotherapy in hepatocellular carcinoma: A bibliometric and knowledge-map analysis.Front Oncol. 2023 Jan 4;12:1071860. doi: 10.3389/fonc.2022.1071860. eCollection 2022. Front Oncol. 2023. PMID: 36686799 Free PMC article.
-
Hepatic arterial infusion chemotherapy with or without lenvatinib for unresectable cholangiocarcinoma: a single-center retrospective study.Hepat Oncol. 2023 Sep 29;10(2):HEP49. doi: 10.2217/hep-2023-0006. eCollection 2023 Jun. Hepat Oncol. 2023. PMID: 37850031 Free PMC article.
-
Hepatic arterial infusion chemotherapy versus transarterial chemoembolization in patients with unresectable intrahepatic cholangiocarcinoma: a multicenter retrospective cohort study.Eur Radiol. 2025 Apr 11. doi: 10.1007/s00330-025-11557-6. Online ahead of print. Eur Radiol. 2025. PMID: 40216615
-
Locoregional Therapy for Intrahepatic Cholangiocarcinoma.Cancers (Basel). 2023 Apr 20;15(8):2384. doi: 10.3390/cancers15082384. Cancers (Basel). 2023. PMID: 37190311 Free PMC article. Review.
References
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous