

Pancreatic Leiomyosarcoma With Schistosomiasis Hematobia: A Case Report and Literature Review
- PMID: 33869026
- PMCID: PMC8045707
- DOI: 10.3389/fonc.2021.638905
Pancreatic Leiomyosarcoma With Schistosomiasis Hematobia: A Case Report and Literature Review
Abstract
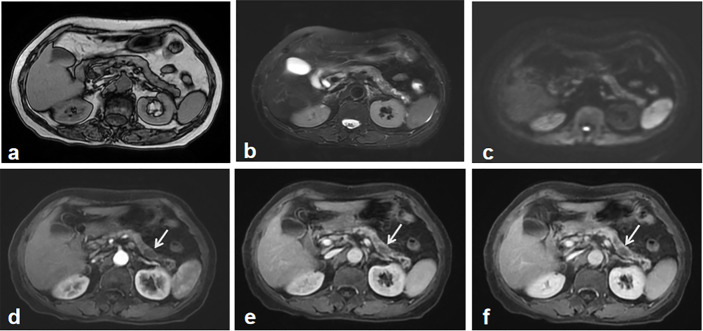
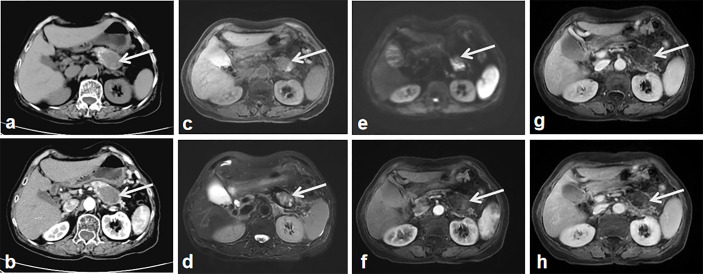
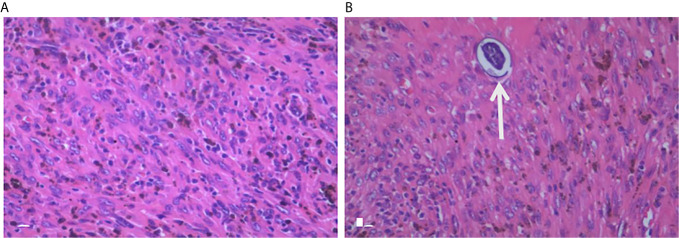
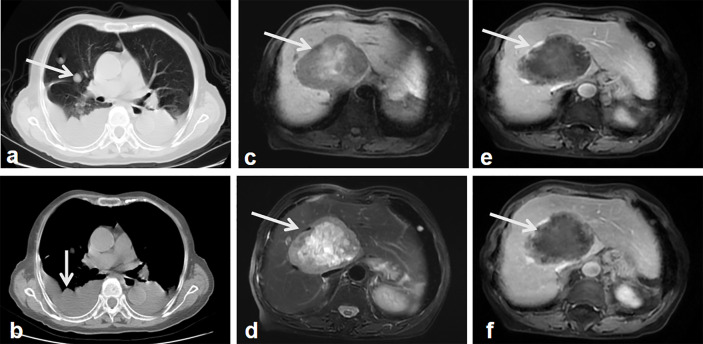
Pancreatic leiomyosarcoma (PL) is a very rare, malignant neoplasm with a very poor prognosis. Here, we examine a novel case of PL with schistosomiasis hematobia. The patient had been initially misdiagnosed by the first magnetic resonance imaging (MRI). The second imaging examination demonstrated an enlarged heterogeneous tumor mass in the body-tail of pancreas. Following image analysis, the patient underwent a pancreatectomy, splenectomy and lymph node dissections. Sixteen months after the tumor resection, follow-up computed tomography (CT) and MRI revealed tumor metastasis in the liver and lung. PL has non-specific clinical manifestations and imaging characteristics, making early diagnosis very challenging. When it is difficult to distinguish between benign and malignant pancreatic lesions, short-term imaging follow-up is preferred. In this case report, we discuss the relationship between PL and schistosomiasis hematobia.
Keywords: differential diagnosis; imaging; metastasis; pancreatic leiomyosarcoma; schistosomiasis hematobia.
Copyright © 2021 Li, Staiculescu, Zhou and Chen.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources