

Krüppel-Like Factor 15 Modulates CXCL1/CXCR2 Signaling-Mediated Inflammatory Response Contributing to Angiotensin II-Induced Cardiac Remodeling
- PMID: 33869197
- PMCID: PMC8047332
- DOI: 10.3389/fcell.2021.644954
Krüppel-Like Factor 15 Modulates CXCL1/CXCR2 Signaling-Mediated Inflammatory Response Contributing to Angiotensin II-Induced Cardiac Remodeling
Abstract
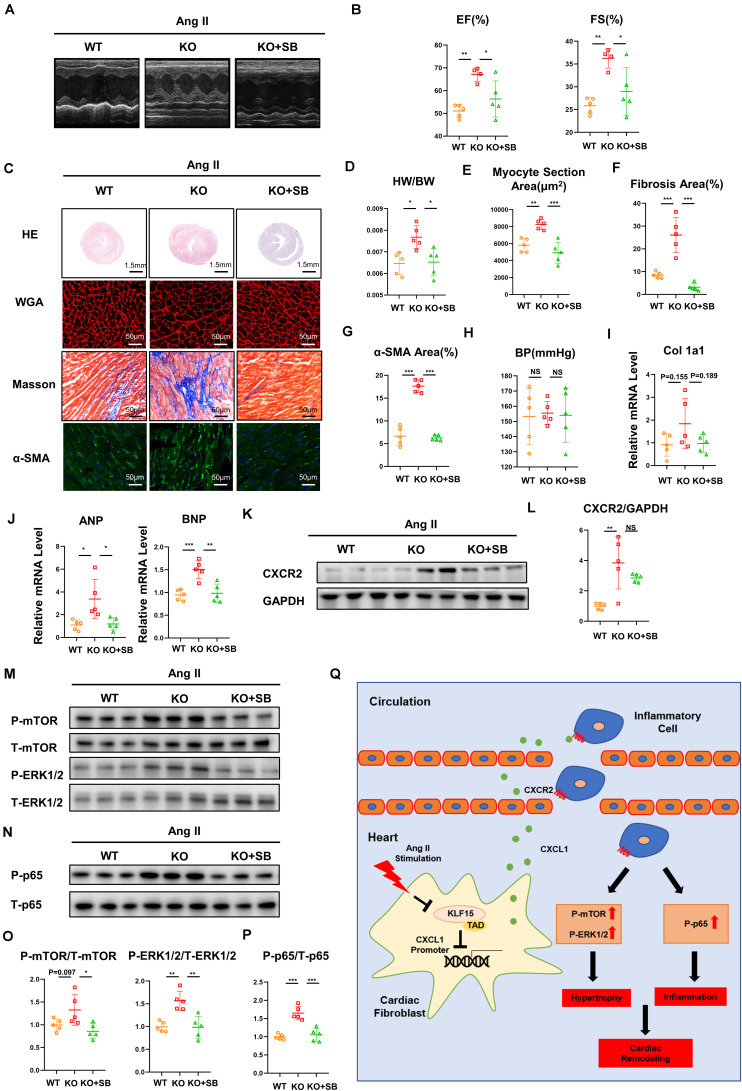
Inflammation is involved in cardiac remodeling. In response to pathological stimuli, activated cardiac fibroblasts (CFs) secreting inflammatory cytokines and chemokines play an important role in monocyte/macrophage recruitment. However, the precise mechanism of CF-mediated inflammatory response in hypertension-induced cardiac remodeling remains unclear. In the present study, we investigated the role of transcription factor Krüppel-like factor 15 (KLF15) in this process. We found that KLF15 expression decreased while chemokine CXCL1 and its receptor CXCR2 expression increased in the hearts of angiotensin II (Ang II)-infused mice. Compared to the wild-type mice, KLF15 knockout (KO) mice aggravated Ang II-induced cardiac hypertrophy and fibrosis. Deficiency of KLF15 promoted macrophage accumulation, increase of CXCL1 and CXCR2 expression, and mTOR, ERK1/2, NF-κB-p65 signaling activation in the hearts. Mechanistically, Ang II dose- dependently decreased KLF15 expression and increased CXCL1 secretion from cardiac fibroblasts but not cardiac myoblasts. Loss- or gain-of-function studies have shown that KLF15 negatively regulated CXCL1 expression through its transactivation domain (TAD). Intriguingly, the adenovirus-mediated full length of KLF15-but not KLF15 with TAD deletion overexpression-markedly prevented pathological change in Ang II-infused mice. Notably, the administration of CXCR2 inhibitor SB265610 reversed KLF15 knockout-mediated aggravation of cardiac dysfunction, remodeling, and inflammation induced by Ang II. In conclusion, our study identifies that KLF15 in cardiac fibroblasts negatively regulates CXCL1/CXCR2 axis-mediated inflammatory response and subsequent cardiac remodeling in hypertension.
Keywords: cardiac remodeling; hypertension; inflammation; renin-angiotensin system; transcription factor.
Copyright © 2021 He, Lu, Guo, Li, Lu, Shao, Zhou, Wang, Wang, Gao and Li.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures





Similar articles
-
Transactivation domain of Krüppel-like factor 15 negatively regulates angiotensin II-induced adventitial inflammation and fibrosis.FASEB J. 2019 May;33(5):6254-6268. doi: 10.1096/fj.201801809R. Epub 2019 Feb 18. FASEB J. 2019. PMID: 30776250
-
CXCL1-CXCR2 axis mediates angiotensin II-induced cardiac hypertrophy and remodelling through regulation of monocyte infiltration.Eur Heart J. 2018 May 21;39(20):1818-1831. doi: 10.1093/eurheartj/ehy085. Eur Heart J. 2018. PMID: 29514257
-
Krüppel-Like Factor 15/Interleukin 11 Axis-Mediated Adventitial Remodeling Depends on Extracellular Signal-Regulated Kinases 1 and 2 Activation in Angiotensin II-Induced Hypertension.J Am Heart Assoc. 2021 Aug 17;10(16):e020554. doi: 10.1161/JAHA.120.020554. Epub 2021 Aug 5. J Am Heart Assoc. 2021. PMID: 34350769 Free PMC article.
-
A Review of CXCL1 in Cardiac Fibrosis.Front Cardiovasc Med. 2021 Apr 28;8:674498. doi: 10.3389/fcvm.2021.674498. eCollection 2021. Front Cardiovasc Med. 2021. PMID: 33996954 Free PMC article.
-
Krüppel-like factor 15 in liver diseases: Insights into metabolic reprogramming.Front Pharmacol. 2023 Mar 2;14:1115226. doi: 10.3389/fphar.2023.1115226. eCollection 2023. Front Pharmacol. 2023. PMID: 36937859 Free PMC article. Review.
Cited by
-
Gpnmb and Spp1 mark a conserved macrophage injury response masking fibrosis-specific programming in the lung.JCI Insight. 2024 Dec 20;9(24):e182700. doi: 10.1172/jci.insight.182700. JCI Insight. 2024. PMID: 39509324 Free PMC article.
-
Effect of KLF15-Mediated Circadian Rhythm on Myocardial Infarction: A Narrative Review.Int J Mol Sci. 2025 May 18;26(10):4831. doi: 10.3390/ijms26104831. Int J Mol Sci. 2025. PMID: 40429972 Free PMC article. Review.
-
Epigenetic Repression of Chloride Channel Accessory 2 Transcription in Cardiac Fibroblast: Implication in Cardiac Fibrosis.Front Cell Dev Biol. 2021 Nov 12;9:771466. doi: 10.3389/fcell.2021.771466. eCollection 2021. Front Cell Dev Biol. 2021. PMID: 34869368 Free PMC article.
-
Targeting WWP1 ameliorates cardiac ischemic injury by suppressing KLF15-ubiquitination mediated myocardial inflammation.Theranostics. 2023 Jan 1;13(1):417-437. doi: 10.7150/thno.77694. eCollection 2023. Theranostics. 2023. PMID: 36593958 Free PMC article.
-
Elabela blunts doxorubicin-induced oxidative stress and ferroptosis in rat aortic adventitial fibroblasts by activating the KLF15/GPX4 signaling.Cell Stress Chaperones. 2023 Jan;28(1):91-103. doi: 10.1007/s12192-022-01317-6. Epub 2022 Dec 13. Cell Stress Chaperones. 2023. PMID: 36510036 Free PMC article.
References
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous