

Renal Involvement in IgG4-Related Disease: From Sunlight to Twilight
- PMID: 33869249
- PMCID: PMC8044528
- DOI: 10.3389/fmed.2021.635706
Renal Involvement in IgG4-Related Disease: From Sunlight to Twilight
Abstract
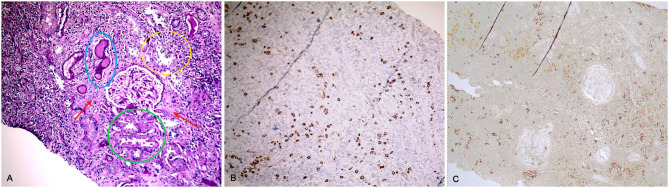
IgG4-Related Disease (IgG4-RD) is a fibroinflammatory condition characterized by a typical histopathological pattern (dense lymphoplasmacytic infiltrate with prevalent IgG4+ plasma cells and storiform fibrosis), which may involve the kidney both directly (IgG4-related kidney disease, IgG4-RKD) or indirectly, as a consequence of post-renal ureteral obstruction due to retroperitoneal fibrosis (IgG4-RD RF). The most frequent presentation of IgG4-RKD is IgG4-related tubulointerstitial nephritis (TIN), but a glomerular disease can be present, in most of the cases a membranous nephropathy. Albeit steroid-responsive, in some cases renal manifestations may lead to progressive and permanent organ damage. In this review we describe four clinical cases representative of typical and less typical renal manifestations of IgG4-RD, emphasizing a potential, subclinical, early involvement of the kidney in the disease.
Keywords: ANCA - associated vasculitis; IgG4-related disease; membranous nephropathy; retroperitoneal fibrosis; tubulointerstitial nephritis (TIN).
Copyright © 2021 Capecchi, Giannese, Moriconi, Bonadio, Pratesi, Croia, Egidi, Puxeddu, Tavoni and Migliorini.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures


References
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous