

Feasibility of ultrathin endoscope for esophageal endoscopic submucosal dissection
- PMID: 33869734
- PMCID: PMC8043804
- DOI: 10.1055/a-1352-3805
Feasibility of ultrathin endoscope for esophageal endoscopic submucosal dissection
Abstract
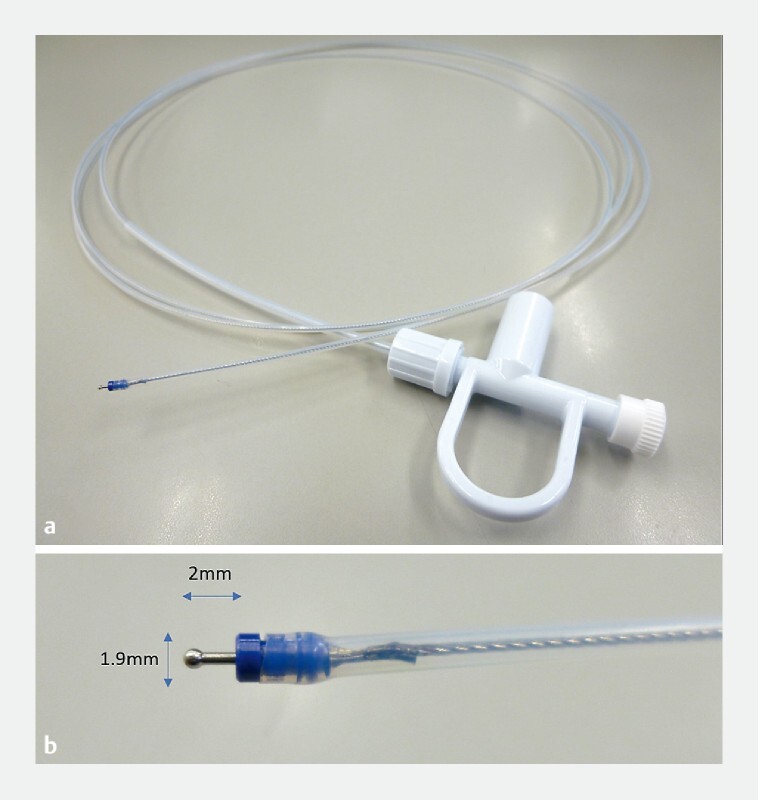
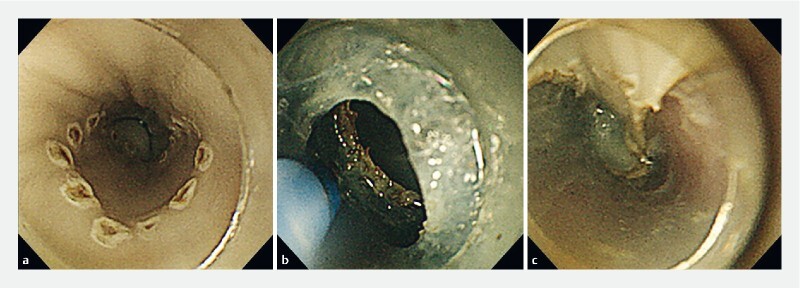
Background and study aims Endoscopic submucosal dissection (ESD) is widely performed for superficial esophageal cancer, but stricture after extensive resection is a major clinical problem. Using an ultrathin endoscope would enable endoscopists to approach lesions beyond the stricture. We evaluated the feasibility of an ultrathin endoscope for esophageal ESD. Methods To perform ESD with an ultrathin endoscope, we developed a transparent hood and ESD knife. A total of 24 esophageal ESDs were performed by two endoscopists with excised and live porcine esophaguses. A GIF-Q260 J and Dual knife were used in the conventional group and the GIF-XP260NS and a newly developed knife were used in the ultrathin group. En bloc resection rates, perforation rates, and procedure times were compared. Results All 24 lesions were resected en bloc without perforation. The mean procedure time was longer in the ultrathin group, although not significantly so (274.3 ± 81.8 s vs 435.8 ± 313.9 s, respectively; P = 0.22). Conclusion Although the procedure time was longer in the ultrathin group, en bloc resection was performed without any perforation. The findings indicate that esophageal ESD with an ultrathin endoscope is feasible.
The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/).
Conflict of interest statement
Competing interests The authors declare that they have no conflict of interest.
Figures

References
-
- Hoteya S, Iizuka T, Kikuchi D et al. Benefits of endoscopic submucosal dissection according to size and location of gastric neoplasm, compared with conventional mucosal resection. J Gastroenterol Hepatol. 2009;24:1102–1106. - PubMed
-
- Yamaguchi N, Isomoto H, Nakayama T et al. Usefulness of oral prednisolone in the treatment of esophageal stricture after endoscopic submucosal dissection for superficial esophageal squamous cell carcinoma. Gastrointest Endosc. 2011;73:1115–1121. - PubMed
-
- Hanaoka N, Ishihara R, Takeuchi Y et al. Intralesional steroid injection to prevent stricture after endoscopic submucosal dissection for esophageal cancer: a controlled prospective study. Endoscopy. 2012;44:1007–1011. - PubMed
-
- Iizuka T, Kikuchi D, Yamada A et al. Polyglycolic acid sheet application to prevent esophageal stricture after endoscopic submucosal dissection for esophageal squamous cell carcinoma. Endoscopy. 2015;47:341–344. - PubMed
-
- Ohki T, Yamato M, Ota M et al. Prevention of esophageal stricture after endoscopic submucosal dissection using tissue-engineered cell sheets. Gastroenterology. 2012;143:582–588. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous