

Ergonomic advantage of pistol-grip endoscope in the ENT practice
- PMID: 33869757
- PMCID: PMC8035956
- DOI: 10.1002/lio2.542
Ergonomic advantage of pistol-grip endoscope in the ENT practice
Abstract
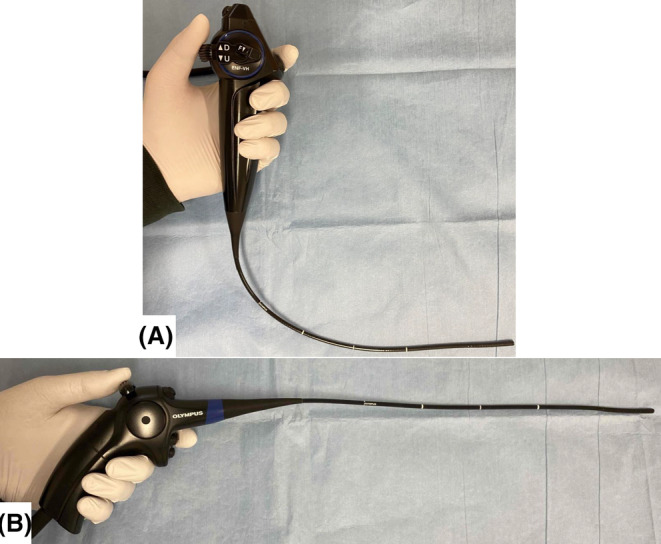
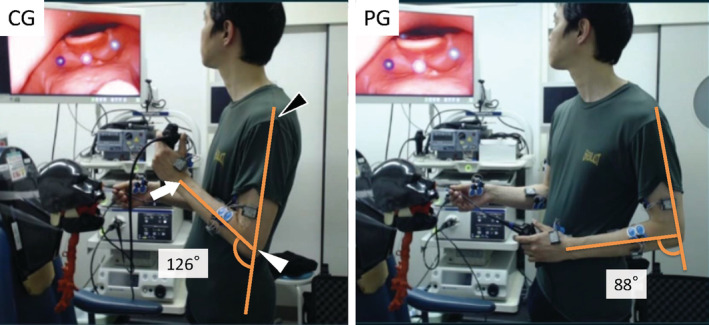
Objectives: Recent technology manufactured a nasopharyngeal videoscope with pistol-shaped grip (PG). This study aimed to assess the ergonomic feasibility of this novel device in daily ENT practice.
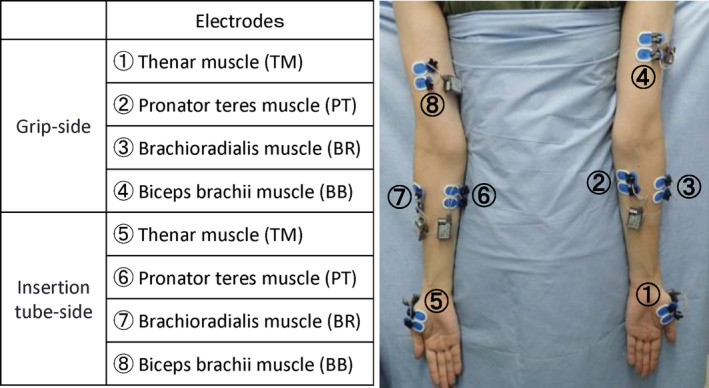
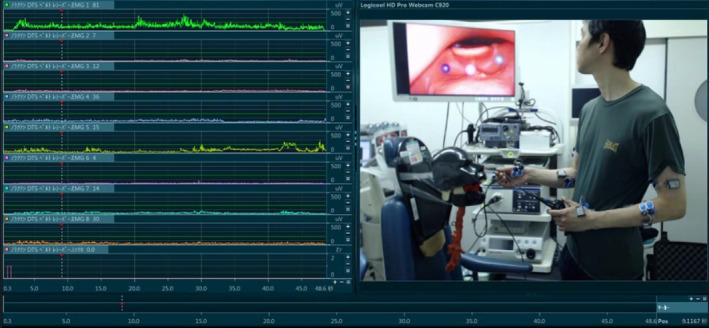
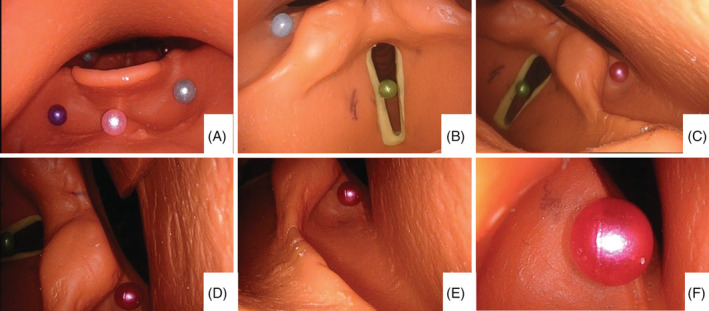
Methods: To assess the ergonomic impact of grip shape on ENT physicians, conventional grip videoscope (CG) and PG were utilized in this study. Surface electromyography (sEMG) was recorded to assess the muscle activity in the upper limb during endoscopy on a training model. Bilateral sEMG recordings were performed including thenar muscle, pronator teres muscle, brachioradialis muscle, and biceps brachii muscle. Mean value of the mean sEMG amplitude throughout the task in triplicated examinations (mMA) with each electrode, total values of four mMAs in both of the grip-side and the insertion tube-side limb muscles, and total value of all eight mMAs were calculated, and compared between CG and PG. Subgroup analyses were also performed in the experienced ENT physicians and the residents.
Results: PG provided significantly lower mMA values in thenar muscle and brachioradialis muscle of the grip-side limb compared with CG. Total value of four mMAs in PG was significantly lower compared with that in CG in the grip-side limb, and total value of all eight mMAs in PG was significantly lower compared with that in CG. Furthermore, total value of four mMAs in PG was significantly lower compared with that in CG in the grip-side limb, in both of the subgroups.
Conclusion: This is the first study to support the idea that the newly designed pistol-grip endoscope may have an ergonomic advantage over conventional endoscope for otolaryngologists in daily practice.
Level of evidence: 4.
Keywords: ENT practice; electromyography; ergonomics; nasopharyngeal endoscopy.
© 2021 The Authors. Laryngoscope Investigative Otolaryngology published by Wiley Periodicals LLC on behalf of The Triological Society.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

Similar articles
-
The effect of ergonomic laparoscopic tool handle design on performance and efficiency.Surg Endosc. 2015 Sep;29(9):2500-5. doi: 10.1007/s00464-014-4005-9. Epub 2014 Dec 24. Surg Endosc. 2015. PMID: 25537377
-
Effect of structured training in improving the ergonomic stress in laparoscopic surgery among general surgery residents.Surg Endosc. 2021 Aug;35(8):4825-4833. doi: 10.1007/s00464-020-07945-2. Epub 2020 Sep 1. Surg Endosc. 2021. PMID: 32875411
-
The Effects of the Biceps Brachii and Brachioradialis on Elbow Flexor Muscle Strength and Spasticity in Stroke Patients.Neural Plast. 2022 Mar 2;2022:1295908. doi: 10.1155/2022/1295908. eCollection 2022. Neural Plast. 2022. PMID: 35283993 Free PMC article.
-
Design and ergonomic evaluation of a new adapted endoscope holder to reduce muscle pressure and discomfort during endoscopy.Work. 2023;76(1):403-410. doi: 10.3233/WOR-220185. Work. 2023. PMID: 36776095
-
Ergonomic interventions for preventing work-related musculoskeletal disorders of the upper limb and neck among office workers.Cochrane Database Syst Rev. 2018 Oct 23;10(10):CD008570. doi: 10.1002/14651858.CD008570.pub3. Cochrane Database Syst Rev. 2018. PMID: 30350850 Free PMC article.
Cited by
-
Using wearable technology for Posture Regulation to Improve Surgical Ergonomics in the paediatric operating room: the UPRISE trial: a pilot study.Surg Endosc. 2024 Aug;38(8):4445-4456. doi: 10.1007/s00464-024-10933-5. Epub 2024 Jun 20. Surg Endosc. 2024. PMID: 38902409 Free PMC article. Clinical Trial.
-
Ergonomics of Various Modalities for Ear Surgery.OTO Open. 2024 Jul 4;8(3):e162. doi: 10.1002/oto2.162. eCollection 2024 Jul-Sep. OTO Open. 2024. PMID: 38974181 Free PMC article.
-
Electrode Size and Placement for Surface EMG Bipolar Detection from the Brachioradialis Muscle: A Scoping Review.Sensors (Basel). 2021 Nov 3;21(21):7322. doi: 10.3390/s21217322. Sensors (Basel). 2021. PMID: 34770627 Free PMC article.
-
Work-Related Musculoskeletal Disorders in Endoscopic Sinus and Skull Base Surgery: A Systematic Review With Meta-analysis.Otolaryngol Head Neck Surg. 2024 Dec;171(6):1650-1669. doi: 10.1002/ohn.892. Epub 2024 Jul 6. Otolaryngol Head Neck Surg. 2024. PMID: 38971976 Free PMC article.
References
-
- Arezes PM, Dinis‐Carvalho J, Alves AC. Workplace ergonomics in lean production environments: a literature review. Work. 2015;52(1):57‐70. - PubMed
-
- Jaffar N, Abdul‐Tharim AH, Mohd‐Kamar IF, Lop NS. A literature review of ergonomics risk factors in construction industry. Procedia Eng. 2011;20:89‐97.
-
- McCaig RH, Gooderson CY. Ergonomic and physiological aspects of military operations in a cold wet climate. Ergonomics. 1986;29(7):849‐857. - PubMed
-
- Hulme A, Thompson J, Plant KL, et al. Applying systems ergonomics methods in sport: a systematic review. Appl Ergon. 2019;80:214‐225. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous