

Impact of Simulation-based Mastery Learning on Resident Skill Managing Mechanical Ventilators
- PMID: 33870322
- PMCID: PMC8043263
- DOI: 10.34197/ats-scholar.2020-0023OC
Impact of Simulation-based Mastery Learning on Resident Skill Managing Mechanical Ventilators
Abstract
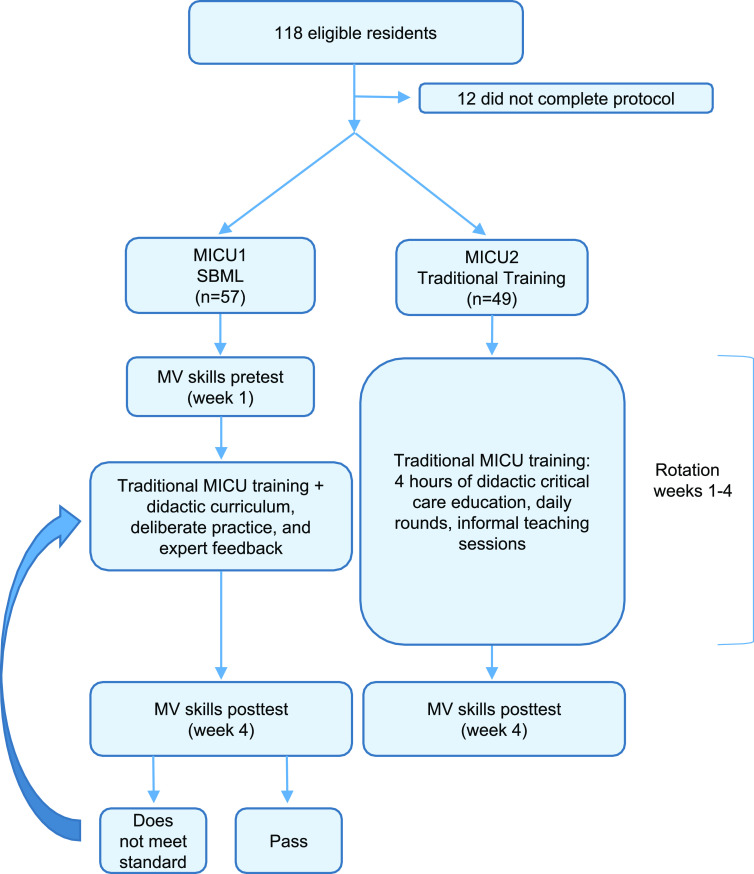
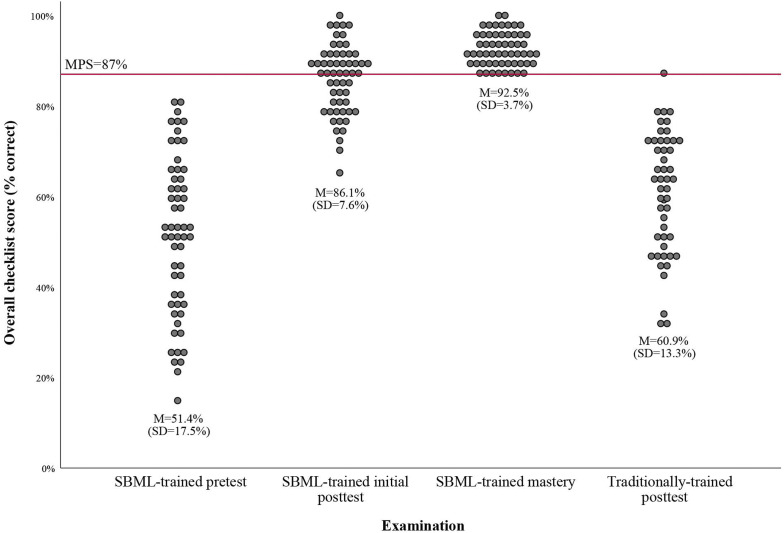
Background: Caring for patients requiring mechanical ventilation is complex, and residents may lack adequate skill for managing these patients. Simulation-based mastery learning (SBML) is an educational model that trains clinicians to a high standard and can reduce complications. The mastery learning model has not been applied to ventilator management. Objective: The purpose of this study was to determine whether SBML, as compared with traditional training, is an effective strategy for teaching residents the skills necessary to manage patients requiring mechanical ventilation. Methods: We developed an SBML curriculum and a 47-item skills checklist to test ventilator management for patients with normal, restricted, and obstructed lung physiology. A minimum passing standard (MPS) on the checklist was set using the Mastery Angoff method. Residents rotating through the medical intensive care unit in Academic Year 2017-2018 were assigned to SBML or traditional training based on their medical intensive care unit team. The SBML group was pretested on a ventilator simulator using the skills checklist. They then received a 1.5-hour session (45 min didactic and 45 min deliberate practice on the simulator with feedback). At rotation completion, they were posttested on the simulator using the checklist until the MPS was met. Both SBML-trained and traditionally trained groups received teaching during daily bedside rounds and twice weekly didactic lectures. At rotation completion, traditionally trained residents were tested using the same skills checklist on the simulator. We compared pretest and posttest performance among SBML-trained residents and end of the rotation test performances between the SBML-trained and traditionally trained residents. Results: The MPS was set at 87% on the checklist. Fifty-seven residents were assigned to the SBML-trained group and 49 were assigned to the traditionally trained group. Mean checklist scores for SBML-trained residents improved from 51.4% (standard deviation [SD] = 17.5%) at pretest to 86.1% (SD = 7.6%) at initial posttest and 92.5% (SD = 3.7%) at final (mastery) posttest (both P < 0.001). Forty-two percent of residents required more than one attempt at the posttest to meet or exceed the MPS. At rotation completion, the traditionally trained residents had a mean test score of 60.9% (SD = 13.3%). Conclusion: SBML is an effective strategy to train residents on mechanical ventilator management. An SBML curriculum may augment traditional training methods to further equip residents to safely manage ventilated patients.
Keywords: assessment; critical care; mechanical ventilation; medical education.
Copyright © 2021 by the American Thoracic Society.
Figures
Comment in
-
Enhancing Resident Skills in Mechanical Ventilation. What Do Residents Learn during Intensive Care Unit Rotations?ATS Sch. 2021 Mar 30;2(1):1-4. doi: 10.34197/ats-scholar.2021-0012ED. ATS Sch. 2021. PMID: 33871485 Free PMC article. No abstract available.
Similar articles
-
Impact of Simulation-based Mastery Learning on Management of Massive Hemoptysis.ATS Sch. 2024 Mar 15;5(2):322-331. doi: 10.34197/ats-scholar.2023-0120IN. eCollection 2024 Jun 1. ATS Sch. 2024. PMID: 39055331 Free PMC article.
-
Simulation-based Mastery Learning Improves Critical Care Skills of Advanced Practice Providers.ATS Sch. 2023 Jan 23;4(1):48-60. doi: 10.34197/ats-scholar.2022-0065OC. eCollection 2023 Mar. ATS Sch. 2023. PMID: 37089675 Free PMC article.
-
Use of a simulation-based mastery learning curriculum for neurology residents to improve the identification and management of status epilepticus.Epilepsy Behav. 2020 Oct;111:107247. doi: 10.1016/j.yebeh.2020.107247. Epub 2020 Jun 27. Epilepsy Behav. 2020. PMID: 32603805
-
Simulation-based mastery learning in gastrointestinal endoscopy training.World J Gastrointest Endosc. 2022 Sep 16;14(9):512-523. doi: 10.4253/wjge.v14.i9.512. World J Gastrointest Endosc. 2022. PMID: 36186944 Free PMC article. Review.
-
Beyond the simulation laboratory: a realist synthesis review of clinical outcomes of simulation-based mastery learning.Acad Med. 2015 Nov;90(11):1553-60. doi: 10.1097/ACM.0000000000000938. Acad Med. 2015. PMID: 26375271 Review.
Cited by
-
Developing Simulation-Based Mastery Learning Curricula for Emergency Medicine Skills Training.AEM Educ Train. 2025 Jun 12;9(3):e70058. doi: 10.1002/aet2.70058. eCollection 2025 Jun. AEM Educ Train. 2025. PMID: 40521339
-
Simulation-based mastery improves nursing skills in BSc nursing students: a quasi-experimental study.BMC Nurs. 2021 Jan 6;20(1):10. doi: 10.1186/s12912-020-00532-9. BMC Nurs. 2021. PMID: 33407420 Free PMC article.
-
Simulation in Mechanical Ventilation Training: Integrating Best Practices for Effective Education.Respir Care. 2024 Oct 25;69(11):1468-1476. doi: 10.4187/respcare.12551. Respir Care. 2024. PMID: 39455249 No abstract available.
-
Assessing Mechanical Ventilation Management Skills: More Tools for the Toolbox.ATS Sch. 2022 Jun 30;3(2):167-170. doi: 10.34197/ats-scholar.2022-0043ED. eCollection 2022 Jun. ATS Sch. 2022. PMID: 35924194 Free PMC article. No abstract available.
-
Simulation-based Assessment to Measure Proficiency in Mechanical Ventilation among Residents.ATS Sch. 2022 Jun 30;3(2):204-219. doi: 10.34197/ats-scholar.2021-0130OC. eCollection 2022 Jun. ATS Sch. 2022. PMID: 35924199 Free PMC article.
References
-
- Pham T, Brochard LJ, Slutsky AS. Mechanical ventilation: state of the art. Mayo Clin Proc. 2017;92:1382–1400. - PubMed
-
- Chudgar SM, Cox CE, Que LG, Andolsek K, Knudsen NW, Clay AS. Current teaching and evaluation methods in critical care medicine: has the Accreditation Council for Graduate Medical Education affected how we practice and teach in the intensive care unit? Crit Care Med. 2009;37:49–60. - PubMed
-
- Cox CE, Carson SS, Ely EW, Govert JA, Garrett JM, Brower RG, et al. Effectiveness of medical resident education in mechanical ventilation. Am J Respir Crit Care Med. 2003;167:32–38. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
