

Impact of Novel Multiinstitutional Curriculum on Critical Care Fellow Ventilator Knowledge
- PMID: 33870325
- PMCID: PMC8043266
- DOI: 10.34197/ats-scholar.2020-0034OC
Impact of Novel Multiinstitutional Curriculum on Critical Care Fellow Ventilator Knowledge
Abstract
Background: Management of mechanical ventilation (MV) is a curricular milestone for trainees in pulmonary critical care medicine (PCCM) and critical care medicine (CCM) fellowships. Though recognition of ventilator waveform abnormalities that could result in patient complications is an important part of management, it is unclear how well fellows recognize these abnormalities.
Objective: To study proficiency of ventilator waveform analysis among first-year fellows enrolled in a MV course compared with that of traditionally trained fellows.
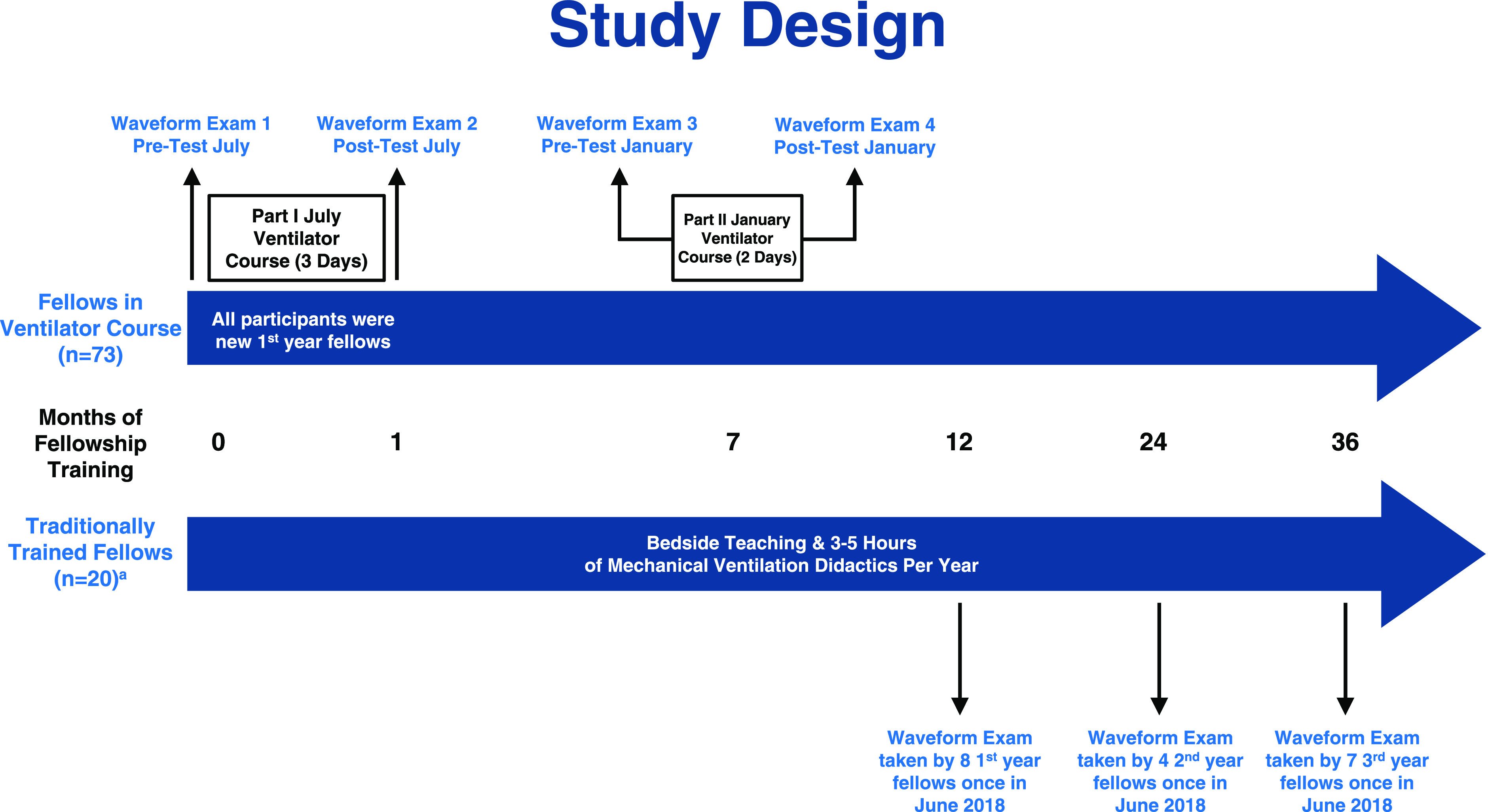
Methods: The study took place from July 2016 to January 2019, with 93 fellows from 10 fellowship programs completing the waveform examination. Seventy-three fellows participated in a course during their first year of fellowship, with part I occurring at the beginning of fellowship in July and part II occurring after 6 months of clinical work. These fellows were given a five-question ventilator waveform examination at multiple time points throughout the two-part course. Twenty fellows from three other fellowship programs who were in their first, second, or third year of fellowship and who did not participate in this course served as the control group. These fellows took the waveform examination a single time, at a median of 23 months into their training.
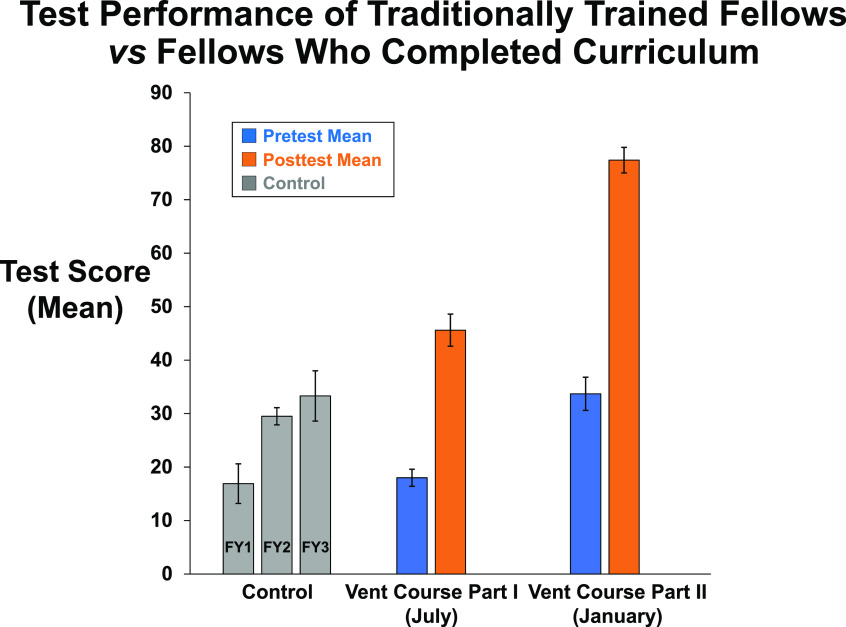
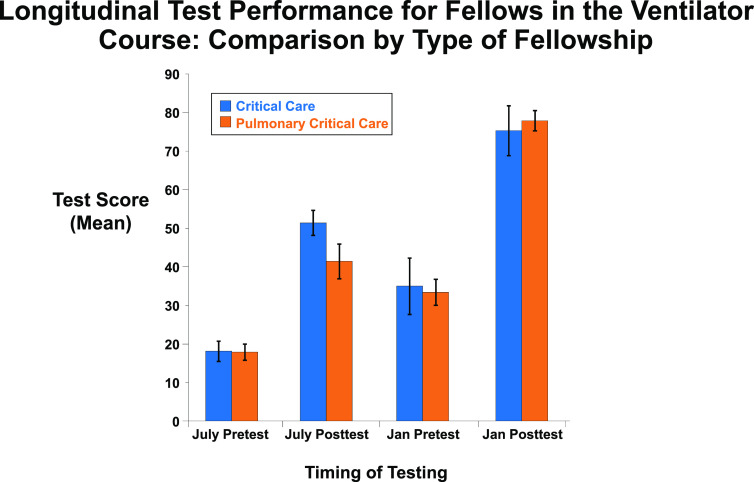
Results: Before the course, scores were low but improved after 3 days of education at the beginning of the fellowship (18.0 ± 1.6 vs. 45.6 ± 3.0; P < 0.0001). Scores decreased after 6 months of clinical rotations but increased to their highest levels after part II of the course (33.7 ± 3.1 for part II pretest vs. 77.4 ± 2.4 for part II posttest; P < 0.0001). After completing part I at the beginning of fellowship, fellows participating in the course outperformed control fellows, who received a median of 23 months of traditional fellowship training at the time of testing (45.6 ± 3.0 vs. 25.3 ± 2.7; P < 0.0001). There was no difference in scores between PCCM and CCM fellows. In anonymous surveys, the fellows also rated the mechanical ventilator lectures highly.
Conclusion: PCCM and CCM fellows do not recognize common waveform abnormalities at the beginning of fellowship but can be trained to do so. Traditional fellowship training may be insufficient to master ventilator waveform analysis, and a more intentional, structured course for MV may help fellowship programs meet the curricular milestones for MV.
Keywords: critical care; fellowship education; mechanical ventilation; waveform analysis.
Copyright © 2021 by the American Thoracic Society.
Figures
Similar articles
-
Impact of Longitudinal Mechanical Ventilation Curriculum on Decay of Knowledge.ATS Sch. 2024 Oct 30;5(2):302-310. doi: 10.34197/ats-scholar.2023-0051IN. eCollection 2024 Jun 1. ATS Sch. 2024. PMID: 39479530 Free PMC article.
-
A Novel Ambulatory Curriculum for Pulmonary and Critical Care Fellowship Training.ATS Sch. 2021 Jun 30;2(2):265-277. doi: 10.34197/ats-scholar.2020-0162OC. eCollection 2021 Jun. ATS Sch. 2021. PMID: 34409420 Free PMC article.
-
Effectiveness of hands-on tutoring and guided self-directed learning versus self-directed learning alone to educate critical care fellows on mechanical ventilation - a pilot project.Med Educ Online. 2016 Sep 29;21:32727. doi: 10.3402/meo.v21.32727. eCollection 2016. Med Educ Online. 2016. PMID: 27702433 Free PMC article.
-
The Society of Gynecologic Oncology wellness curriculum pilot: A groundbreaking initiative for fellowship training.Gynecol Oncol. 2020 Mar;156(3):710-714. doi: 10.1016/j.ygyno.2019.12.005. Epub 2020 Jan 3. Gynecol Oncol. 2020. PMID: 31911007 Review.
-
Gender, Race, and Ethnic Representation of Incoming Transplant Hepatology Fellows: A 14-Year Analysis of Fellowship Diversity.Gastro Hep Adv. 2023 Apr 26;2(6):765-767. doi: 10.1016/j.gastha.2023.04.007. eCollection 2023. Gastro Hep Adv. 2023. PMID: 39130124 Free PMC article. Review. No abstract available.
Cited by
-
Comparison of Web-Based and On-Site Lung Simulators for Education in Mechanical Ventilation.Respir Care. 2024 Oct 25;69(11):1353-1360. doi: 10.4187/respcare.12072. Respir Care. 2024. PMID: 39379159 Clinical Trial.
-
Emergency and critical care medicine residents' competency to identify patient ventilator asynchrony using a mechanical ventilator waveform analysis in Addis Ababa, Ethiopia: a multicenter cross-sectional study.BMC Med Educ. 2025 Feb 4;25(1):180. doi: 10.1186/s12909-025-06748-0. BMC Med Educ. 2025. PMID: 39905426 Free PMC article.
-
Survey of Ventilator Waveform Interpretation Among ICU Professionals.Respir Care. 2024 Jun 28;69(7):773-781. doi: 10.4187/respcare.11677. Respir Care. 2024. PMID: 38653558 Free PMC article.
-
Impact of a Competency-based Mechanical Ventilation Course Using Virtual Simulation.ATS Sch. 2025 Jun;6(2):202-216. doi: 10.34197/ats-scholar.2024-0083OC. Epub 2025 Feb 18. ATS Sch. 2025. PMID: 39964256 Free PMC article.
-
Simulation-based Assessment to Measure Proficiency in Mechanical Ventilation among Residents.ATS Sch. 2022 Jun 30;3(2):204-219. doi: 10.34197/ats-scholar.2021-0130OC. eCollection 2022 Jun. ATS Sch. 2022. PMID: 35924199 Free PMC article.
References
-
- Wilcox SR, Seigel TA, Strout TD, Schneider JI, Mitchell PM, Marcolini EG, et al. Emergency medicine residents’ knowledge of mechanical ventilation. J Emerg Med. 2015;48:481–491. - PubMed
-
- Barrett ML, Smith MW, Elixhauser A, Honigman LS, Pines JM. Healthcare Cost and Utilization Project (HCUP) statistical briefs. Rockville, MD: Agency for Healthcare Research and Quality (US); 2014. Utilization of intensive care services 2011: statistical brief #185. - PubMed
-
- Fessler HE, Addrizzo-Harris D, Beck JM, Buckley JD, Pastores SM, Piquette CA, et al. Entrustable professional activities and curricular milestones for fellowship training in pulmonary and critical care medicine: report of a multisociety working group. Chest. 2014;146:813–834. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
