

Associations of Skeletal Muscle Mass and Fat Mass With Incident Cardiovascular Disease and All-Cause Mortality: A Prospective Cohort Study of UK Biobank Participants
- PMID: 33870707
- PMCID: PMC8200765
- DOI: 10.1161/JAHA.120.019337
Associations of Skeletal Muscle Mass and Fat Mass With Incident Cardiovascular Disease and All-Cause Mortality: A Prospective Cohort Study of UK Biobank Participants
Abstract
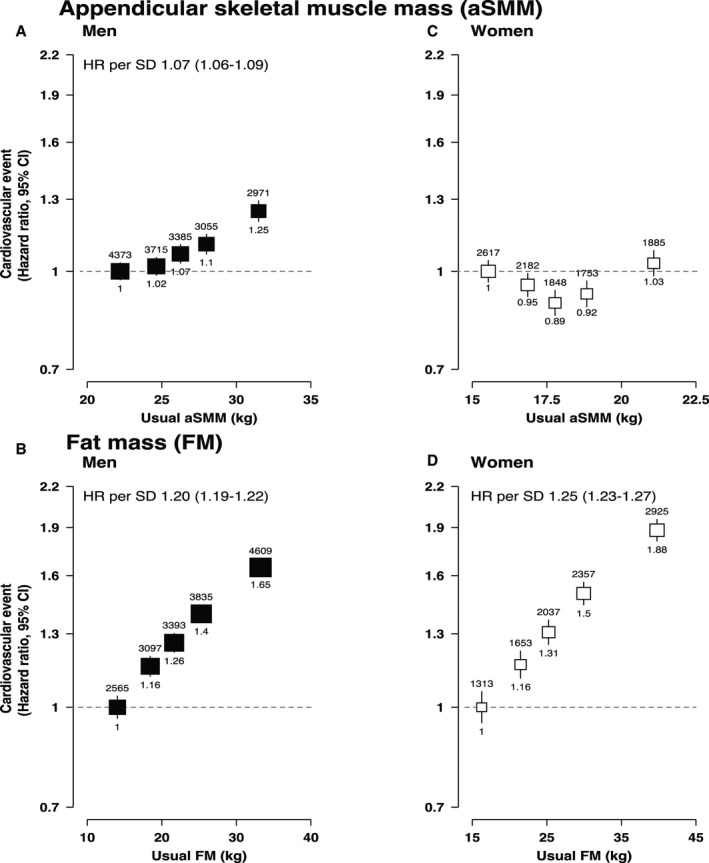
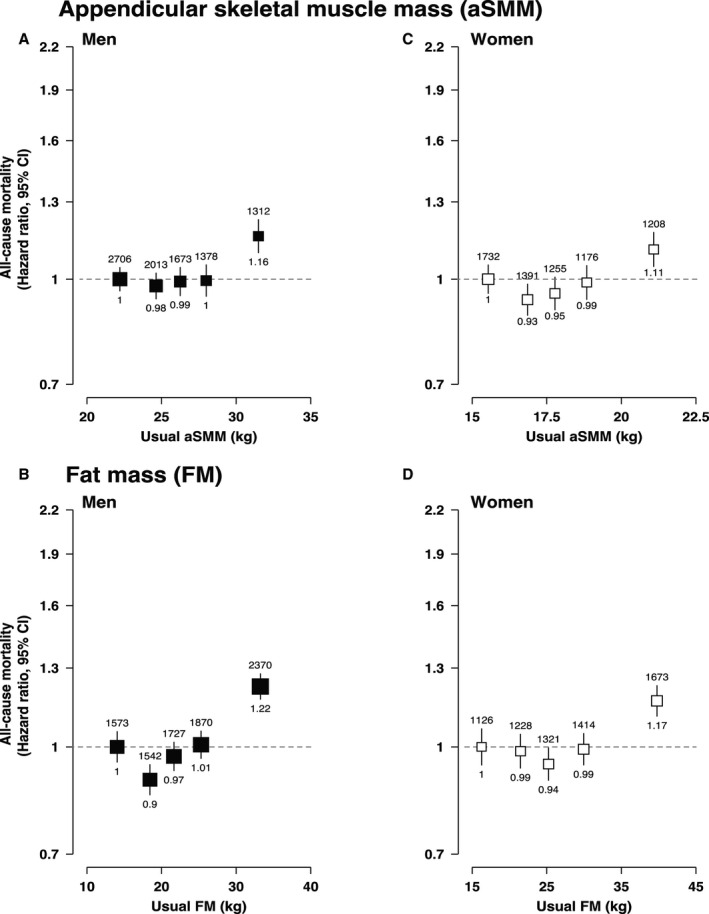
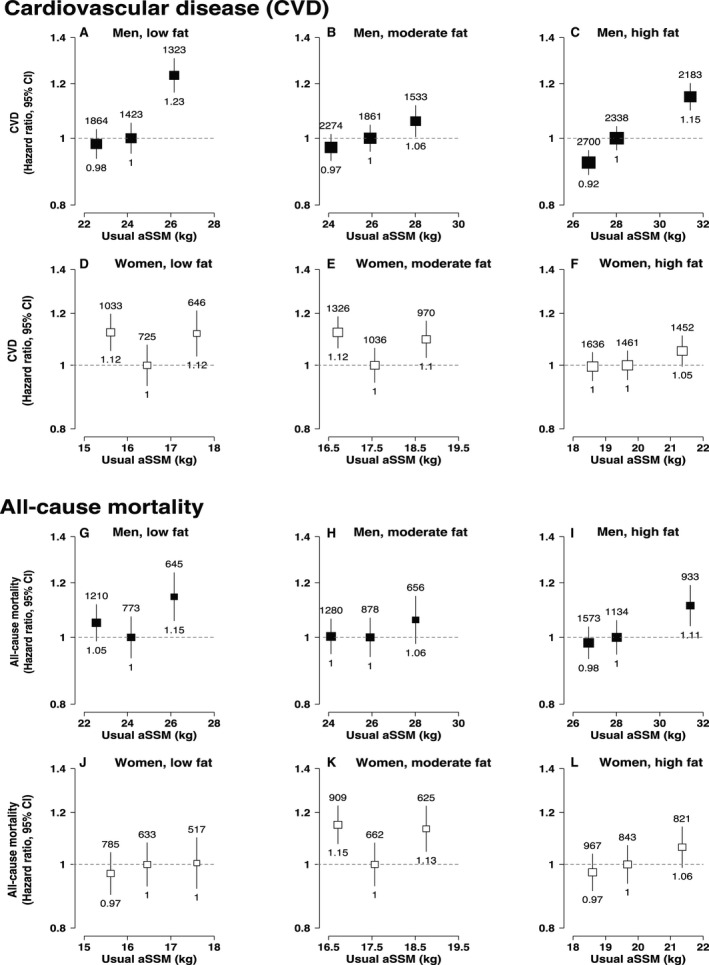
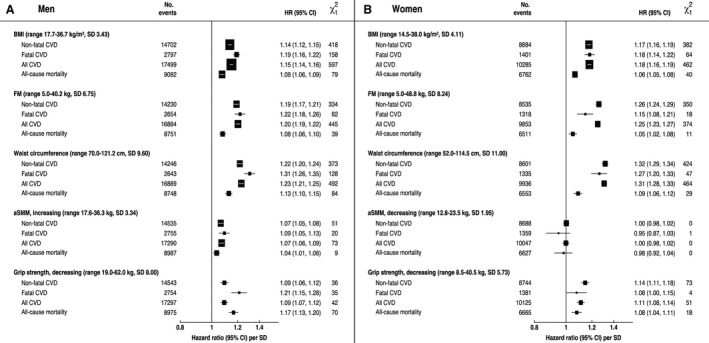
Background There is debate whether body mass index is a good predictor of health outcomes because different tissues, namely skeletal muscle mass (SMM) and fat mass (FM), may be differentially associated with risk. We investigated the association of appendicular SMM (aSMM) and FM with fatal and nonfatal cardiovascular disease (CVD) and all-cause mortality. We compared their prognostic value to that of body mass index. Methods and Results We studied 356 590 UK Biobank participants aged 40 to 69 years with bioimpedance analysis data for whole-body FM and predicted limb muscle mass (to calculate aSMM). Associations between aSMM and FM with CVD and all-cause mortality were examined using multivariable Cox proportional hazards models. Over 3 749 501 person-years of follow-up, there were 27 784 CVD events and 15 844 all-cause deaths. In men, aSMM was positively associated with CVD incidence (hazard ratio [HR] per 1 SD 1.07; 95% CI, 1.06-1.09) and there was a curvilinear association in women. There were stronger positive associations between FM and CVD with HRs per SD of 1.20 (95% CI, 1.19-1.22) and 1.25 (95% CI, 1.23-1.27) in men and women respectively. Within FM tertiles, the associations between aSMM and CVD risk largely persisted. There were J-shaped associations between aSMM and FM with all-cause mortality in both sexes. Body mass index was modestly better at discriminating CVD risk. Conclusions FM showed a strong positive association with CVD risk. The relationship of aSMM with CVD risk differed between sexes, and potential mechanisms need further investigation. Body fat and SMM bioimpedance measurements were not superior to body mass index in predicting population-level CVD incidence or all-cause mortality.
Keywords: all‐cause mortality; cardiovascular disease; cohort study; fat mass; skeletal muscle mass.
Conflict of interest statement
None.
Figures
References
-
- Yusuf S, Hawken S, Ounpuu S, Dans T, Avezum A, Lanas F, McQueen M, Budaj A, Pais P, Varigos J, et al. Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART study): case control study. Lancet. 2004;364:937–952. DOI: 10.1016/S0140-6736(04)17018-9. - DOI - PubMed
-
- Whitlock G, Lewington S, Sherliker P, Clarke R, Emberson J, Halsey J, Qizilbash N, Collins R, Peto R, MacMahon S, et al. Body‐mass index and cause‐specific mortality in 900 000 adults: collaborative analyses of 57 prospective studies. Lancet. 2009;373:1083–1096. DOI: 10.1016/S0140-6736(09)60318-4. - DOI - PMC - PubMed
-
- Ng M, Fleming T, Robinson M, Thomson B, Graetz N, Margono C, Mullany EC, Biryukov S, Abbafati C, Abera SF, et al. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980–2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2014;384:766–781. DOI: 10.1016/S0140-6736(14)60460-8. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
