

Impact of Chronic Hypertension and Antihypertensive Treatment on Adverse Perinatal Outcomes: Systematic Review and Meta-Analysis
- PMID: 33870708
- PMCID: PMC8200761
- DOI: 10.1161/JAHA.120.018494
Impact of Chronic Hypertension and Antihypertensive Treatment on Adverse Perinatal Outcomes: Systematic Review and Meta-Analysis
Abstract
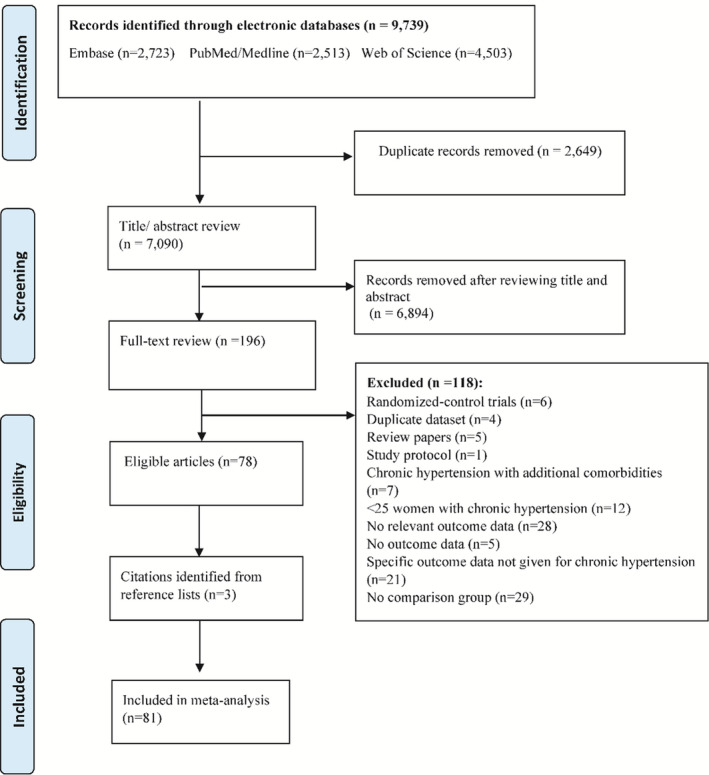
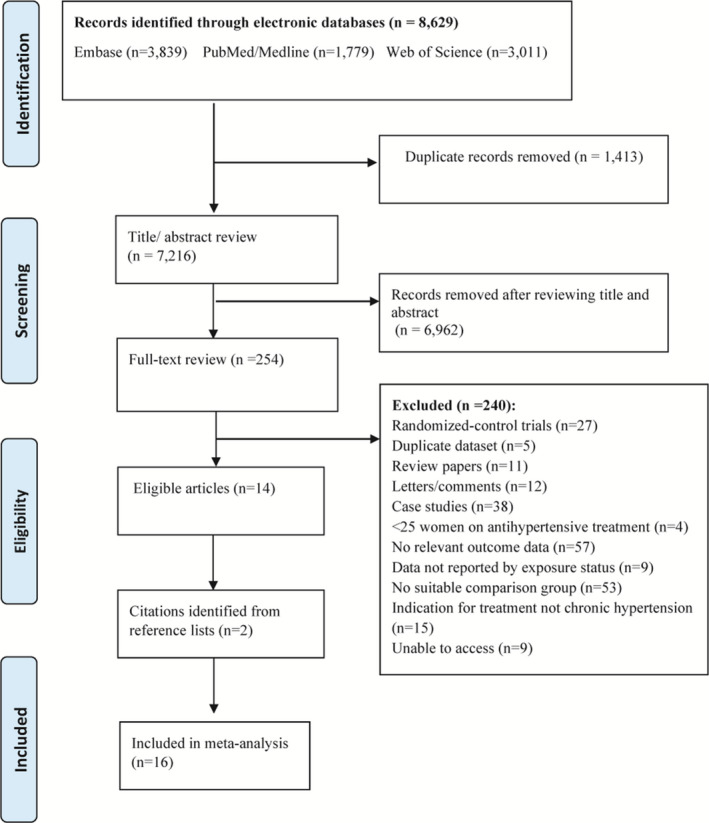
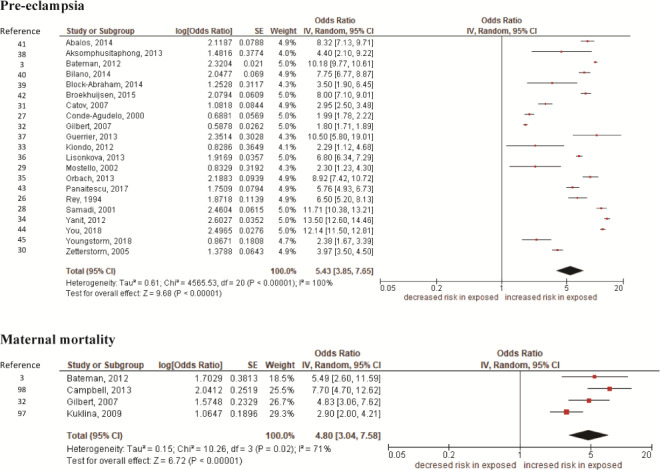
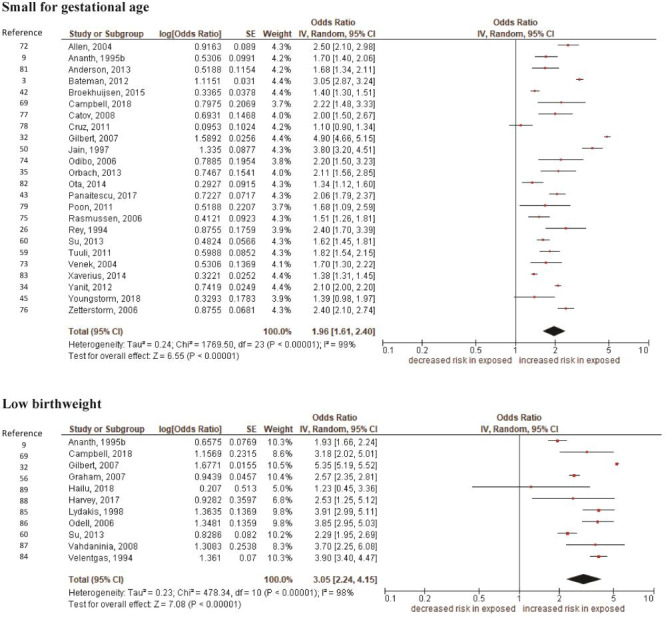
Background Maternal chronic hypertension is associated with adverse pregnancy outcomes. Previous studies examined the association between either chronic hypertension or antihypertensive treatment and adverse pregnancy outcomes. We aimed to synthesize the evidence on the effect of chronic hypertension/antihypertensive treatment on adverse pregnancy outcomes. Methods and Results Medline/PubMed, EMBASE, and Web of Science were searched; we included observational studies and assessed the effect of race/ethnicity, where possible, following a registered protocol (CRD42019120088). Random-effects meta-analyses were used. A total of 81 studies were identified on chronic hypertension, and a total of 16 studies were identified on antihypertensive treatment. Chronic hypertension was associated with higher odds of preeclampsia (adjusted odd ratio [aOR], 5.43; 95% CI, 3.85-7.65); cesarean section (aOR, 1.87; 95% CI, 1.6-2.16); maternal mortality (aOR, 4.80; 95% CI, 3.04-7.58); preterm birth (aOR, 2.23; 95% CI, 1.96-2.53); stillbirth (aOR, 2.32; 95% CI, 2.22-2.42); and small for gestational age (SGA) (aOR, 1.96; 95% CI, 1.6-2.40). Subgroup analyses indicated that maternal race/ethnicity does not influence the observed associations. Women with chronic hypertension on antihypertensive treatment (versus untreated) had higher odds of SGA (aOR, 1.86; 95% CI, 1.38-2.50). Conclusions Chronic hypertension is associated with adverse pregnancy outcomes, and these associations appear to be independent of maternal race/ethnicity. In women with chronic hypertension, those on treatment had a higher risk of SGA, although the number of studies was limited. This could result from a direct effect of the treatment or because severe hypertension during pregnancy is a risk factor for SGA and women with severe hypertension are more likely to be treated. The effect of antihypertensive treatment on SGA needs to be further tested with large randomized controlled trials.
Keywords: antihypertensive; chronic hypertension; fetal outcome; meta‐analysis; neonatal outcome; pregnancy; systematic review.
Conflict of interest statement
None.
Figures
References
-
- Brown MA, Magee LA, Kenny LC, Karumanchi SA, McCarthy FP, Saito S, Hall DR, Warren CE, Adoyi G, Ishaku S. Hypertensive disorders of pregnancy: ISSHP classification, diagnosis, and management recommendations for international practice. Hypertension. 2018;72:24–43. DOI: 10.1161/HYPERTENSIONAHA.117.10803. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
