

Attack rates amongst household members of outpatients with confirmed COVID-19 in Bergen, Norway: A case-ascertained study
- PMID: 33871470
- PMCID: PMC8009692
- DOI: 10.1016/j.lanepe.2020.100014
Attack rates amongst household members of outpatients with confirmed COVID-19 in Bergen, Norway: A case-ascertained study
Abstract
Background: Households studies reflect the natural spread of SARS-CoV-2 in immunologically naive populations with limited preventive measures to control transmission.We hypothesise that seropositivity provides more accurate household attack rates than RT-PCR. Here, we investigated the importance of age in household transmission dynamics.
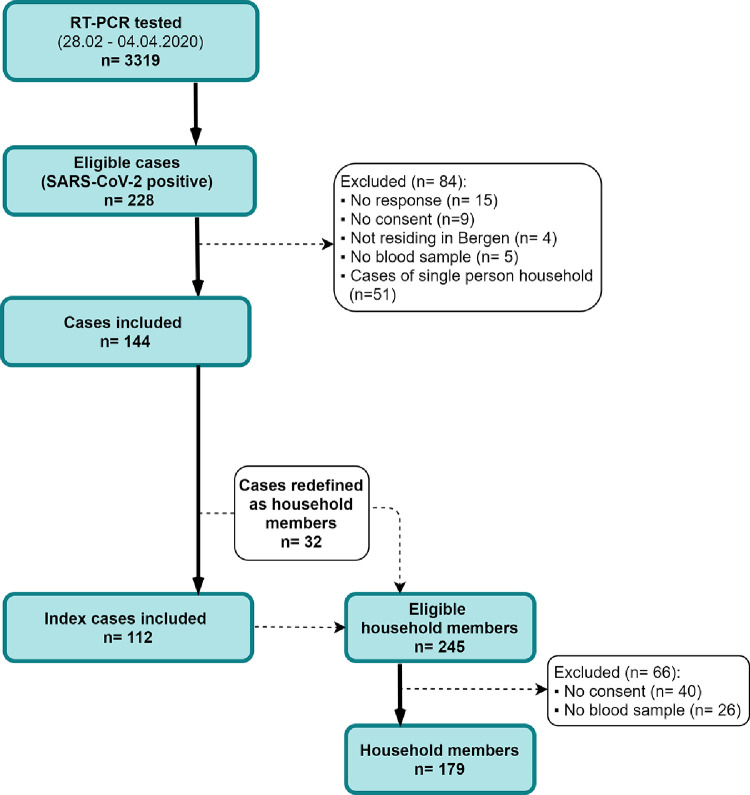
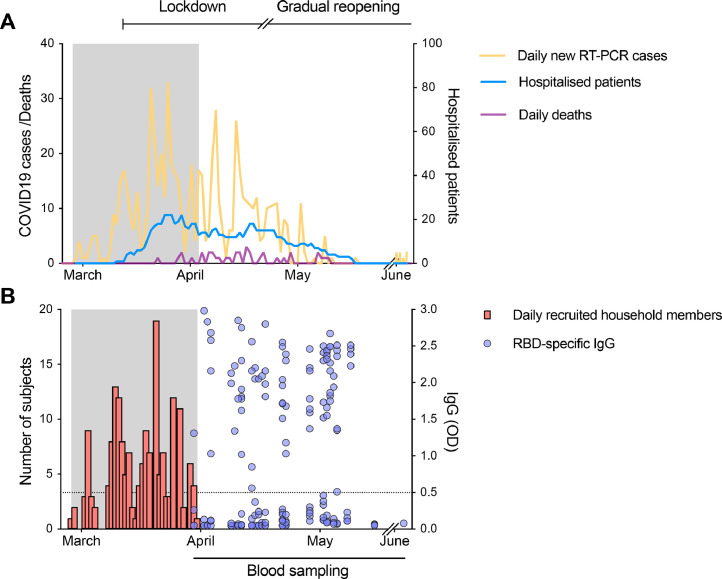
Methods: We enroled 112 households (291 participants) in a case-ascertained study in Bergen, Norway from 28th February to 4th April 2020, collecting demographic and clinical data from index patients and household members. SARS-CoV-2-specific antibodies were measured in sera collected 6-8 weeks after index patient nasopharyngeal testing to define household attack rates.
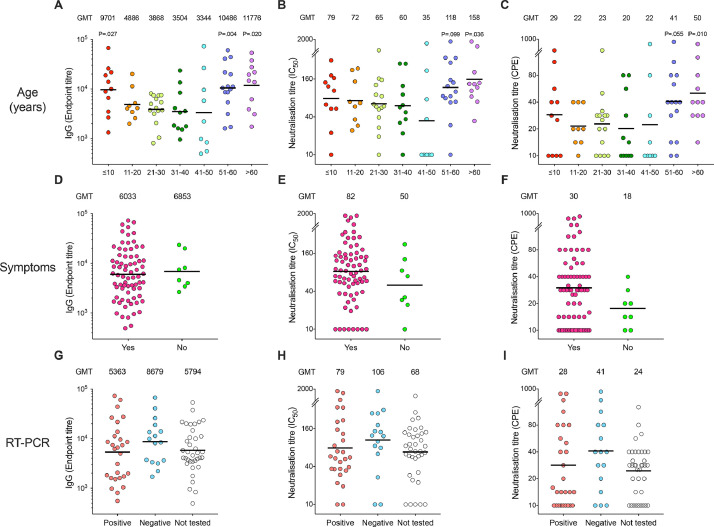
Findings: The overall attack rate was 45% (95% CI 38-53) assessed by serology, and 47% when also including seronegative RT-PCR positives. Serology identified a higher number of infected household members than RT-PCR. Attack rates were equally high in children (48%) and young adults (42%). The attack rate was 16% in asymptomatic household members and 42% in RT-PCR negative contacts. Older adults had higher antibody titres than younger adults. The risk of household transmission was higher when the index patient had fever (aOR 3.31 [95% CI 1.52-7.24]; p = 0.003) or dyspnoea (aOR 2.25 [95% CI 1.80-4.62]; p = 0.027) during acute illness.
Interpretation: Serological assays provide more sensitive and robust estimates of household attack rates than RT-PCR. Children are equally susceptible to infection as young adults. Negative RT-PCR or lack of symptoms are not sufficient to rule out infection in household members.
Funding: Helse Vest (F-11628), Trond Mohn Foundation (TMS2020TMT05).
Bakgrunn: Studier av husstander gjenspeiler den naturlige spredningen av SARS-CoV-2 blant ikke-immune populasjoner med begrensede tiltak for å forebygge smittespredning. Vår hypotese er at antistoff-påvisning gir mer nøyaktige angrepsrater i husstander sammenliknet med RT-PCR. Her undersøker vi betydnignenngen betydningen av alder i smittespredningen.
Metoder: Vi rekrutterte 112 husstander (291 studiedeltakere) i en indeks kasus-bekreftet studie i Bergen, Norge fra 28.02.2020 til 04.04.2020, og samlet inn demografiske og kliniske data fra indekspasienter og deres husstandsmedlemmer. Angrepsrate i husstander ble beregnet ved å måle SARS-CoV-2-spesifikke antistoffer i sera samlet 6–8 uker etter nasofarynksprøve av indekspasienten.
Funn: Den totale angrepsraten var 45% (95% KI 38–53) vurdert ved serologi, og 47% ved å inkludere antistoff negative, RT-PCR positive husstandsmedlemmer. Spesifikke antistoffer identifiserer en høyere andel infiserte husstandsmedlemmer sammenliknet med RT-PCR. Angrepsraten var like høy hos barn (48%) og unge voksne (42%). Angrepsraten var 16% hos personer uten symptomer og 42% hos RT-PCR negative husstandsmedlemmer. Eldre voksne hadde høyere antistoff titre enn yngre voksne. Risiko for smitte i husstander var høyere når indekspasienten hadde feber (aOR 3.31 [95% KI 1.52–7.24]; p = 0.003) eller dyspne (aOR 2.25 [95% KI 1.80–4.62]; p = 0.027) under akuttfasen.
Tolkning: Serologiske analyser gir mer sensitive og robuste estimater av angrepsrate i husstander sammenliknet med RT-PCR. Barn er like utsatt for infeksjon som voksne. Negativ RT-PCR eller fravær av symptomer er ikke tilstrekkelige for å utelukke infeksjon blant husstandsmedlemmer.
Finansiering: Helse Vest (F-11628), Trond Mohn Stiftelse (TMS2020TMT05).
© 2020 The Author(s).
Conflict of interest statement
An ELISA assay used to screen for seroconversion was developed in Florian Krammer´s laboratory. Mount Sinai has filed patent applications to protect that assay and has licensed its use to several companies. Mount Sinai is also commercializing the assay. All other authors declare no conflict of interest.
Figures
References
-
- Organization WHO. WHO Coronavirus disease (COVID-19) dashboard 2020 [Available from: https://covid19.who.int/.
-
- Folkehelseinstituttet. COVID-19 Ukerapport - uke 43 2020 [updated 28th October 2020. Available from: https://www.fhi.no/contentassets/8a971e7b0a3c4a06bdbf381ab52e6157/vedleg....
-
- Folkehelseinstituttet. En person har testet positivt på koronavirus 2020 [Available from: https://www.fhi.no/nyheter/2020/en-person-har-testet-positivt-pa-koronav....
-
- Regjeringen.no . 2020. Omfattende tiltak for å bekjempe koronaviruset 2020. [updated 12th March.
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
