

Evaluation of early postoperative intravenous opioid rescue as a novel quality measure in patients who receive thoracic epidural analgesia: a retrospective cohort analysis and prospective performance improvement intervention
- PMID: 33874890
- PMCID: PMC8054410
- DOI: 10.1186/s12871-021-01332-7
Evaluation of early postoperative intravenous opioid rescue as a novel quality measure in patients who receive thoracic epidural analgesia: a retrospective cohort analysis and prospective performance improvement intervention
Abstract
Background: In this study, we explored the utility of intravenous opioid rescue analgesia in the post anesthesia care unit (PACU-OpResc) as a single marker of thoracic epidural analgesia (TEA) failure and evaluated the resource implications and quality improvement applications of this measure.
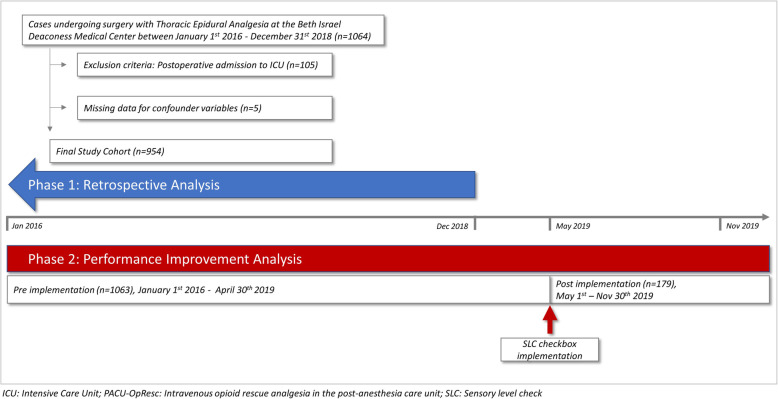
Methods: We performed a retrospective analysis of all TEA placements over a three-year period at a single academic medical center in Boston, Massachusetts. The study exposure was PACU-OpResc. Primary outcome was PACU length of stay (LOS). Secondary outcomes included reasons for delayed PACU discharge and intraoperative hypotension. The analyses were adjusted for confounding variables including patient comorbidities, surgical complexity, intraoperative intravenous opioids, chronic opioid use and local anesthetic bolus through TEA catheter. Post analysis chart review was conducted to determine the positive predictive value (PPV) of PACU-OpResc for inadequate TEA. As a first Plan-Do-Study-Act cycle, we then introduced a checkbox for documentation of a sensory level check after TEA placement. Post implementation data was collected for 7 months.
Results: PACU-OpResc was required by 211 (22.1%) patients who received preoperative TEA, was associated with longer PACU LOS (incidence rate ratio 1.20, 95% CI:1.07-1.34, p = 0.001) and delayed discharge due to inadequate pain control (odds ratio 5.15, 95% CI 3.51-7.57, p < 0.001). PACU-OpResc had a PPV of 76.3 and 60.4% for re-evaluation and manipulation of the TEA catheter in PACU, respectively. Following implementation of a checkbox, average monthly compliance with documented sensory level check after TEA placement was noted to be 39.7%. During this time, a reduction of 8.2% in the rate of PACU-OpResc was observed.
Conclusions: This study demonstrates that PACU-OpResc can be used as a quality assurance measure or surrogate for TEA efficacy, to track performance and monitor innovation efforts aimed at improving analgesia, such as our intervention to facilitate sensory level checks and reduced PACU-OpResc.
Trial registration: not applicable.
Keywords: Efficiency metrics; Perioperative analgesia; Quality improvement; Regional anesthesia; Thoracic epidural analgesia.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures


Similar articles
-
Continuous intraoperative epidural infusions affect recovery room length of stay and analgesic requirements: a single-center observational study.J Anesth. 2017 Aug;31(4):494-501. doi: 10.1007/s00540-017-2316-4. Epub 2017 Feb 9. J Anesth. 2017. PMID: 28185011 Free PMC article.
-
Postoperative analgesia in patients undergoing robot-assisted thoracic surgery: a comparison between thoracic epidural analgesia and intercostal nerve block combined with intravenous patient-controlled analgesia.Ann Palliat Med. 2021 Feb;10(2):1985-1993. doi: 10.21037/apm-20-1607. Epub 2021 Jan 6. Ann Palliat Med. 2021. PMID: 33440971
-
Effects of thoracic epidural anesthesia/analgesia on the stress response, pain relief, hospital stay, and treatment costs of patients with esophageal carcinoma undergoing thoracic surgery: A single-center, randomized controlled trial.Medicine (Baltimore). 2019 Feb;98(7):e14362. doi: 10.1097/MD.0000000000014362. Medicine (Baltimore). 2019. PMID: 30762735 Free PMC article. Clinical Trial.
-
Assessment of Intercostal Nerve Block Analgesia for Thoracic Surgery: A Systematic Review and Meta-analysis.JAMA Netw Open. 2021 Nov 1;4(11):e2133394. doi: 10.1001/jamanetworkopen.2021.33394. JAMA Netw Open. 2021. PMID: 34779845 Free PMC article.
-
Ketamine for perioperative pain management in children: a meta-analysis of published studies.Paediatr Anaesth. 2011 Jun;21(6):636-52. doi: 10.1111/j.1460-9592.2011.03566.x. Epub 2011 Mar 29. Paediatr Anaesth. 2011. PMID: 21447047 Review.
Cited by
-
Effect of Topical Application of an NSAID Lateral to the Incision on Postoperative Pain Following Unicompartmental Knee Arthroplasty: A Double-Blind Randomized Controlled Trial.Orthop Surg. 2024 Jul;16(7):1555-1561. doi: 10.1111/os.14084. Epub 2024 May 28. Orthop Surg. 2024. PMID: 38806283 Free PMC article. Clinical Trial.
-
The association of nitrous oxide on length of stay in the postanesthesia care unit: a retrospective observational study.Can J Anaesth. 2021 Nov;68(11):1630-1640. doi: 10.1007/s12630-021-02067-2. Epub 2021 Aug 18. Can J Anaesth. 2021. PMID: 34406608 English.
References
-
- Manion M.D. SC, Brennan Ph.D., M.D. TJ, Uzan J, Carbonnel M, Piconne O, Asmar R, et al. Thoracic Epidural Analgesia and Acute Pain Management. Anesthesiol J Am Soc Anesthesiol [Internet]. 2011;115(1):467–74. Available from: 10.1097/ALN.0b013e318220847c,. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
