

Evaluating the long-term efficacy and effectiveness of Viscocanalostomy and combined phacoemulsification with Viscocanalostomy in the treatment of patients with uveitic glaucoma: 5-year follow up data
- PMID: 33874928
- PMCID: PMC8056643
- DOI: 10.1186/s12893-021-01176-5
Evaluating the long-term efficacy and effectiveness of Viscocanalostomy and combined phacoemulsification with Viscocanalostomy in the treatment of patients with uveitic glaucoma: 5-year follow up data
Abstract
Background: Uveitic glaucoma commonly leads to a more intense optic nerve damage than other types of glaucoma, causing glaucomatous optic nerves and visual field defects. Anterior uveitis is the most commonly associated risk factor. Surgical intervention is usually indicated when all medical treatment has failed. We report five-year results for 16 eyes of uveitic glaucoma managed with viscocanalostomy (VC)/Phaco viscocanalostomy (PVC).
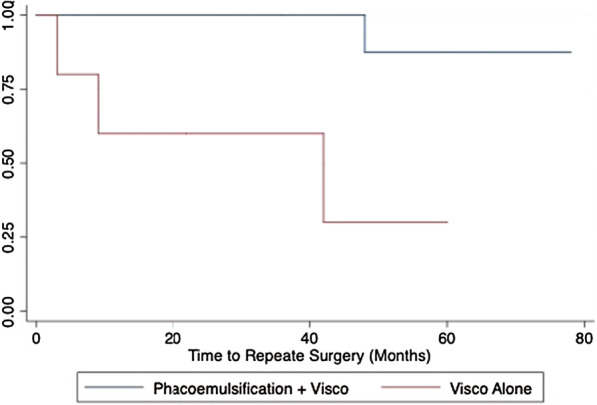
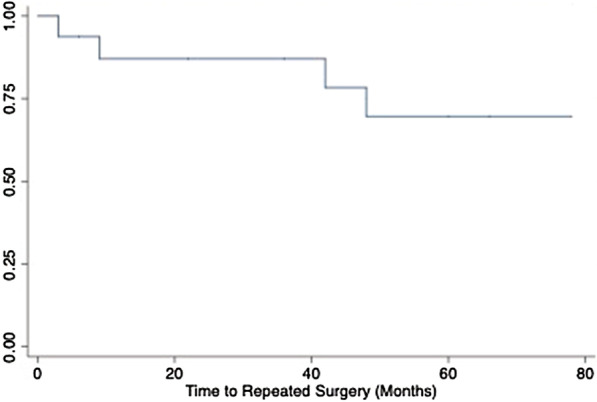
Methods: Retrospective analysis on all uveitic glaucoma cases meeting a five-year follow up was completed. All patients were managed surgically with either viscocanalostomy (VC) or phacoviscocanalostomy (PVC). Outcomes evaluated included intraocular pressures measurement pre-listing, on day 1, year 1 to year 5. Complete success rate was defined as achieving an intraocular pressure (IOP) lower than 21 mmHg or reduced by 30% without medications, and qualified success was achieved when IOP was lower than 21 mmHg or a reduction in IOP of 30% with topical medical therapy ± Laser goniopuncture (LGP). If further surgeries were required to reduce IOP due to glaucoma progression then they were classified as a failure.
Results: A total of 16 patients with uveitic glaucoma were reviewed. Complete success was seen in 75% of patients at year 1, 50% of patients at year 3 and 19% of patients in year 5. Conversely qualified success was achieved in 94% of patients at year 1, 86% of patients at year 3 and 75% of patients at year 5. In the group of patients requiring further surgery, 50% of patients had previous surgeries, including cataract surgery, trabeculectomy and viscocanalostomy. There was a mean number of 4 pre-operative drops before their primary surgery and a mean drop in eye medications of 1.1 at 5 years follow-up. Success rates were prognostically linked to lower mean number of interventions and lower percentage of previous surgeries.
Conclusion: There remains a significant paucity of information in the utilization of PVC in uveitic glaucoma. The advantage of nonpenetrating glaucoma surgery (NPGS) includes the lack of entry into the anterior chamber and the avoidance of an iridectomy which may reduce intraocular inflammation and postoperative complications. Our study shows that non-penetrating surgery is successful in treating advanced uveitic glaucoma.
Keywords: Phaco viscocanalostomy; Uveitic glaucoma; Uveitis; Viscocanalostomy.
Conflict of interest statement
We declare we have received no financial support for the content of this article. The authors declare that they have no competing interests, and no financial arrangements exist which may be interpreted as having the potential to bias the outcome of this case.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
