

The effect of chiropractic care on infantile colic: results from a single-blind randomised controlled trial
- PMID: 33874955
- PMCID: PMC8054384
- DOI: 10.1186/s12998-021-00371-8
The effect of chiropractic care on infantile colic: results from a single-blind randomised controlled trial
Abstract
Background: Chiropractic care is commonly used to treat infantile colic. However large trials with parental blinding are missing. Therefore, the purpose of this study is to evaluate the effect of chiropractic care on infantile colic.
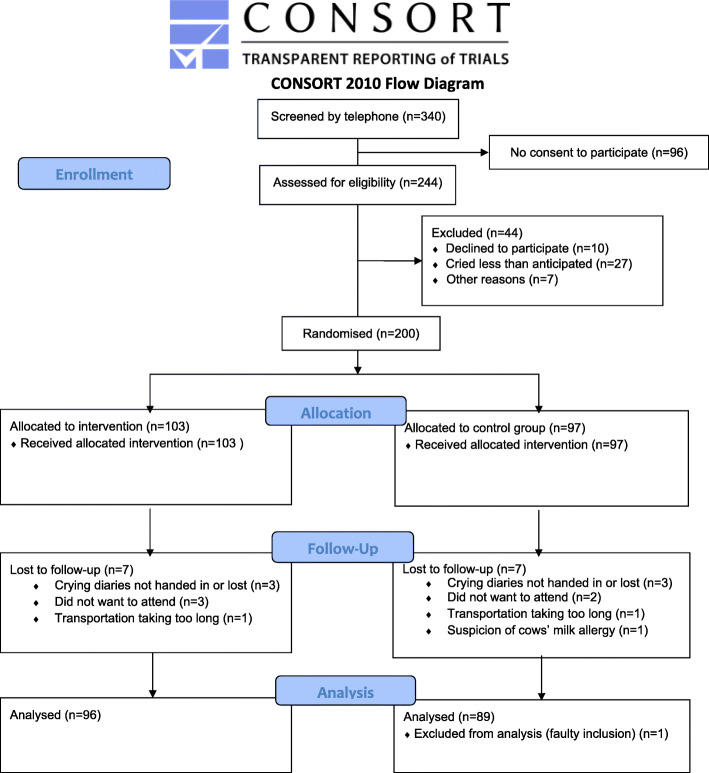
Method: This is a multicenter, single-blind randomized controlled trial conducted in four Danish chiropractic clinics, 2015-2019. Information was distributed in the maternity wards and by maternal and child health nurses. Children aged 2-14 weeks with unexplained excessive crying were recruited through home visits and randomized (1:1) to either chiropractic care or control group. Both groups attended the chiropractic clinic twice a week for 2 weeks. The intervention group received chiropractic care, while the control group was not treated. The parents were not present in the treatment room and unaware of their child's allocation. The primary outcome was change in daily hours of crying before and after treatment. Secondary outcomes were changes in hours of sleep, hours being awake and content, gastrointestinal symptoms, colic status and satisfaction. All outcomes were based on parental diaries and a final questionnaire.
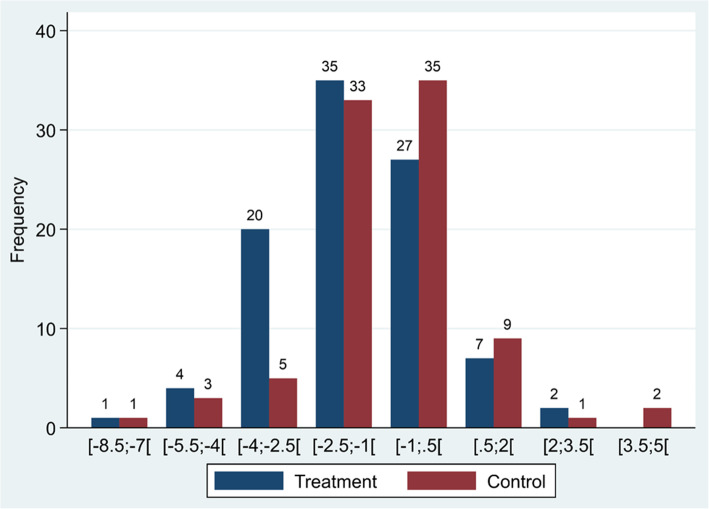
Results: Of 200 recruited children, 185 completed the trial (treatment group n = 96; control group n = 89). Duration of crying in the treatment group was reduced by 1.5 h compared with 1 h in the control group (mean difference - 0.6, 95% CI - 1.1 to - 0.1; P = 0.026), but when adjusted for baseline hours of crying, age and chiropractic clinic, the difference was not significant (P = 0.066). The proportion obtaining a clinically important reduction of 1 h of crying was 63% in the treatment group and 47% in the control group (p = 0.037), and NNT was 6.5. We found no effect on any of the secondary outcomes.
Conclusion: Excessive crying was reduced by half an hour in favor of the group receiving chiropractic care compared with the control group, but not at a statistically significant level after adjustments. From a clinical perspective, the mean difference between the groups was small, but there were large individual differences, which emphasizes the need to investigate if subgroups of children, e.g. those with musculoskeletal problems, benefit more than others from chiropractic care.
Trial registration: Clinical Trials NCT02595515 , registered 2 November 2015.
Keywords: Chiropractic; Excessive crying; Infantile colic; Manipulative treatment; Randomized controlled trial.
Conflict of interest statement
All authors have completed the ICMJE uniform disclosure form at
They declare that LVH has received grants from the Foundation for Chiropractic Research and Postgraduate Education, the European Centre for Chiropractic Research Excellence, the Fund for General Practice, the General Practitioners’ Foundation for Education and Development, and the Research Fund for the Region of Southern Denmark at different times during the project period; LH and HWC have received grants and are supported partly by the Foundation for Chiropractic Research and Postgraduate Education; JS and DJ have no financial relationship with any organisation that might have an interest in the submitted work in the previous 3 years; no other relationship or activities that could appear to have influenced the submitted work.
Figures
Comment in
-
Response to Letter to the Editor: "The effect of chiropractic care on infantile colic: results from a single-blind randomised controlled trial" and "Identifying potential treatment effect modifiers of the effectiveness of chiropractic care to infants with colic through prespecified secondary analyses of a randomised controlled trial".Chiropr Man Therap. 2021 Aug 4;29(1):29. doi: 10.1186/s12998-021-00385-2. Chiropr Man Therap. 2021. PMID: 34348735 Free PMC article. No abstract available.
-
Letter to the Editor: "The effect of chiropractic care on infantile colic: results from a single-blind randomised controlled trial" and "Identifying potential treatment effect modifiers of the effectiveness of chiropractic care to infants with colic through prespecified secondary analyses of a randomised controlled trial".Chiropr Man Therap. 2021 Aug 4;29(1):30. doi: 10.1186/s12998-021-00386-1. Chiropr Man Therap. 2021. PMID: 34348762 Free PMC article. No abstract available.
References
-
- Wessel MA, Cobb JC, Jackson EB, Harris GS, Jr, Detwiler AC. Paroxysmal fussing in infancy, sometimes called colic. Pediatrics. 1954;14(5):421–435. - PubMed
-
- Benninga MA, Faure C, Hyman PE, St James Roberts I, Schechter NL, Nurko S. Childhood functional gastrointestinal disorders: neonate/toddler. Gastroenterology. 2016;S0016-5085(16)00182-7. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
