

Prevention of postoperative delirium through the avoidance of potentially inappropriate medications in a geriatric surgical patient
- PMID: 33875501
- PMCID: PMC8057549
- DOI: 10.1136/bcr-2020-240403
Prevention of postoperative delirium through the avoidance of potentially inappropriate medications in a geriatric surgical patient
Abstract
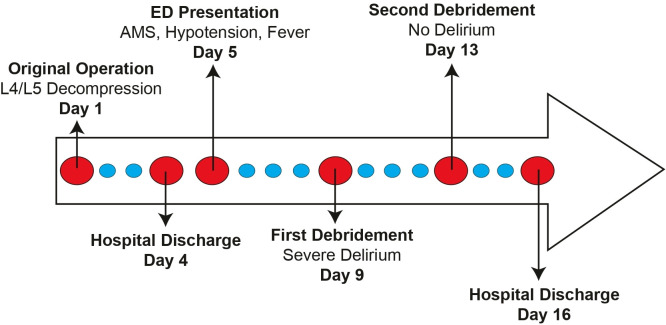
We demonstrate the utility of risk stratification for postoperative delirium in geriatric patients and show that postoperative delirium can be prevented in high-risk patients when potentially inappropriate medications (PIMs) (medications that are best avoided in older adults) are avoided. In this case, a 65-year-old woman underwent two debridement procedures with similar presurgical risk for postoperative delirium. There was no risk stratification or preoperative cognitive assessment in the first procedure, she received PIMs and developed postoperative delirium. In the second procedure, PIMs were intentionally avoided and postoperative delirium did not occur. This case supports recent recommendations from the European Society of Anaesthesiology, the American Society of Anesthesiologists and the American Geriatrics Society that providers assess a patient's cognitive function and delirium risk profile preoperatively to appropriately guide perioperative management.
Keywords: anaesthesia; delirium; geriatric medicine; surgery; unwanted effects / adverse reactions.
© BMJ Publishing Group Limited 2021. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- American Psychiatric Association . Diagnostic and statistical manual of mental disorders. 5th ed. Arlington, VA, 2013.
-
- Lingehall HC, Smulter NS, Lindahl E, et al. Preoperative cognitive performance and postoperative delirium are independently associated with future dementia in older people who have undergone cardiac surgery: a longitudinal cohort study. Crit Care Med 2017;45:1295–303. 10.1097/CCM.0000000000002483 - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical