

Data sharing to improve concordance in variant interpretation across laboratories: results from the Canadian Open Genetics Repository
- PMID: 33875564
- PMCID: PMC8523590
- DOI: 10.1136/jmedgenet-2021-107738
Data sharing to improve concordance in variant interpretation across laboratories: results from the Canadian Open Genetics Repository
Abstract
Background: This study aimed to identify and resolve discordant variant interpretations across clinical molecular genetic laboratories through the Canadian Open Genetics Repository (COGR), an online collaborative effort for variant sharing and interpretation.
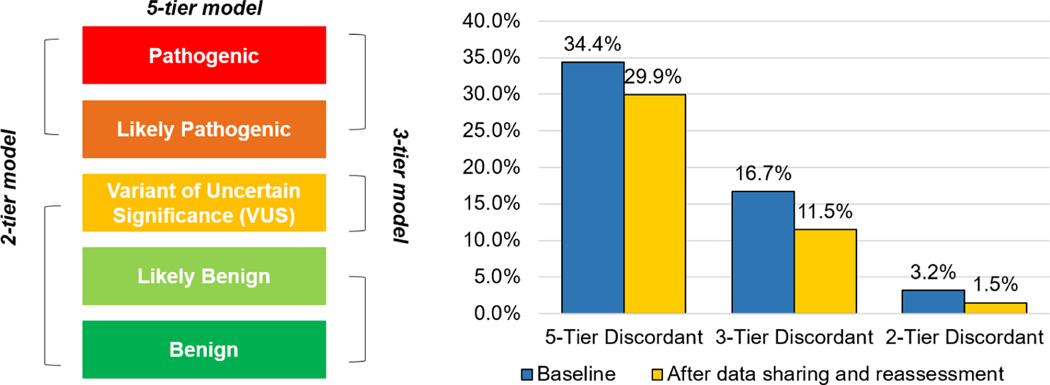
Methods: Laboratories uploaded variant data to the Franklin Genoox platform. Reports were issued to each laboratory, summarising variants where conflicting classifications with another laboratory were noted. Laboratories could then reassess variants to resolve discordances. Discordance was calculated using a five-tier model (pathogenic (P), likely pathogenic (LP), variant of uncertain significance (VUS), likely benign (LB), benign (B)), a three-tier model (LP/P are positive, VUS are inconclusive, LB/B are negative) and a two-tier model (LP/P are clinically actionable, VUS/LB/B are not). We compared the COGR classifications to automated classifications generated by Franklin.
Results: Twelve laboratories submitted classifications for 44 510 unique variants. 2419 variants (5.4%) were classified by two or more laboratories. From baseline to after reassessment, the number of discordant variants decreased from 833 (34.4% of variants reported by two or more laboratories) to 723 (29.9%) based on the five-tier model, 403 (16.7%) to 279 (11.5%) based on the three-tier model and 77 (3.2%) to 37 (1.5%) based on the two-tier model. Compared with the COGR classification, the automated Franklin classifications had 94.5% sensitivity and 96.6% specificity for identifying actionable (P or LP) variants.
Conclusions: The COGR provides a standardised mechanism for laboratories to identify discordant variant interpretations and reduce discordance in genetic test result delivery. Such quality assurance programmes are important as genetic testing is implemented more widely in clinical care.
Keywords: genetic testing; genetics; human genetics.
© Author(s) (or their employer(s)) 2022. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures



References
-
- Richards S, Aziz N, Bale S, Bick D, Das S, Gastier-Foster J, Grody WW, Hegde M, Lyon E, Spector E, Voelkerding K, Rehm HL, ACMG Laboratory Quality Assurance Committee. Standards and guidelines for the interpretation of sequence variants: a joint consensus recommendation of the American College of medical genetics and genomics and the association for molecular pathology. Genet Med 2015;17:405–23. - PMC - PubMed
-
- Mighton C, Charames GS, Wang M, Zakoor K-R, Wong A, Shickh S, Watkins N, Lebo MS, Bombard Y, Lerner-Ellis J. Variant classification changes over time in BRCA1 and BRCA2. Genet Med 2019;21:2248–54. - PubMed
-
- Amendola LM, Jarvik GP, Leo MC, McLaughlin HM, Akkari Y, Amaral MD, Berg JS, Biswas S, Bowling KM, Conlin LK, Cooper GM, Dorschner MO, Dulik MC, Ghazani AA, Ghosh R, Green RC, Hart R, Horton C, Johnston JJ, Lebo MS, Milosavljevic A, Ou J, Pak CM, Patel RY, Punj S, Richards CS, Salama J, Strande NT, Yang Y, Plon SE, Biesecker LG, Rehm HL. Performance of ACMG-AMP Variant-Interpretation guidelines among nine laboratories in the clinical sequencing exploratory research Consortium. Am J Hum Genet 2016;98:1067–76. - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources