

Classical and Counter-Regulatory Renin-Angiotensin System: Potential Key Roles in COVID-19 Pathophysiology
- PMID: 33875979
- PMCID: PMC8046706
- DOI: 10.1016/j.cjco.2021.04.004
Classical and Counter-Regulatory Renin-Angiotensin System: Potential Key Roles in COVID-19 Pathophysiology
Abstract
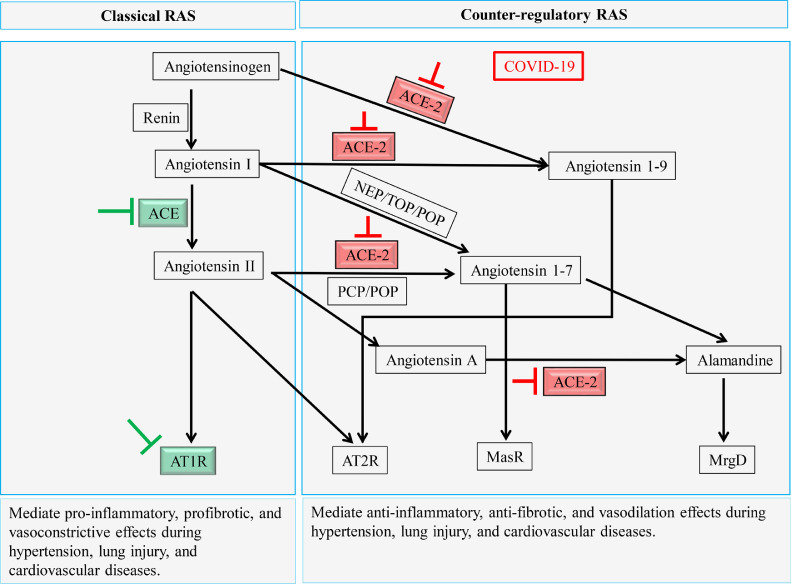
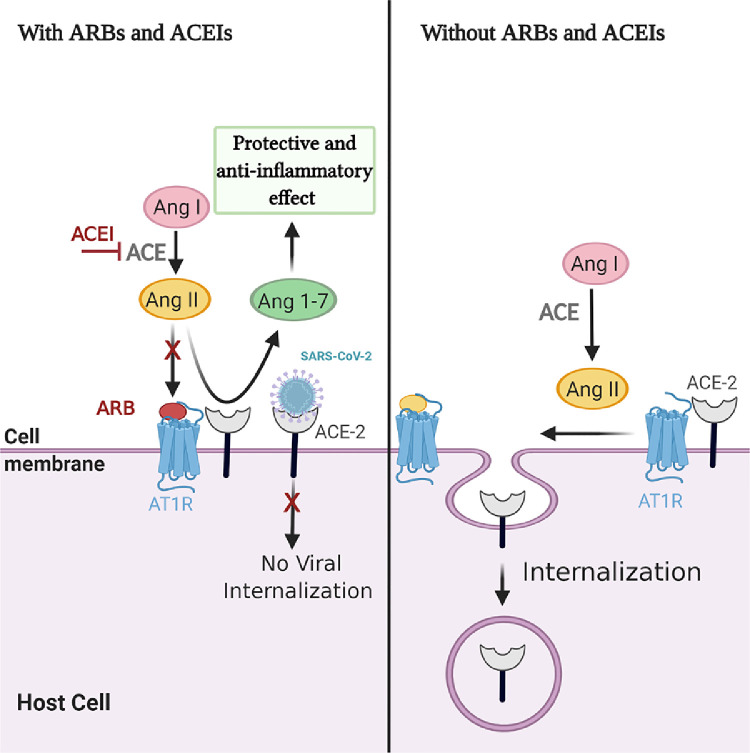
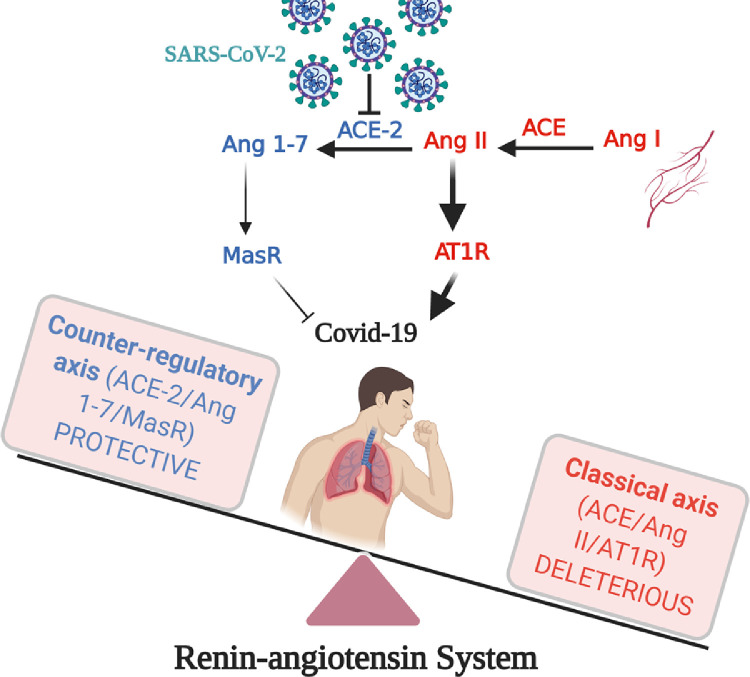
In the current COVID-19 pandemic, severe acute respiratory syndrome coronavirus 2 uses angiotensin-converting enzyme-2 (ACE-2) receptors for cell entry, leading to ACE-2 dysfunction and downregulation, which disturb the balance between the classical and counter-regulatory renin-angiotensin system (RAS) in favor of the classical RAS. RAS dysregulation is one of the major characteristics of several cardiovascular diseases; thus, adjustment of this system is the main therapeutic target. RAS inhibitors-particularly angiotensin-converting enzyme inhibitors (ACEIs) and angiotensin II type 1 receptor blockers (ARBs)-are commonly used for treatment of hypertension and cardiovascular disease. Patients with cardiovascular diseases are the group most commonly seen among those with COVID-19 comorbidity. At the beginning of this pandemic, a dilemma occurred regarding the use of ACEIs and ARBs, potentially aggravating cardiovascular and pulmonary dysfunction in COVID-19 patients. Urgent clinical trials from different countries and hospitals reported that there is no association between RAS inhibitor treatment and COVID-19 infection or comorbidity complication. Nevertheless, the disturbance of the RAS that is associated with COVID-19 infection and the potential treatment targeting this area have yet to be resolved. In this review, the link between the dysregulation of classical RAS and counter-regulatory RAS activities in COVID-19 patients with cardiovascular metabolic diseases is investigated. In addition, the latest findings based on ACEI and ARB administration and ACE-2 availability in relation to COVID-19, which may provide a better understanding of the RAS contribution to COVID-19 pathology, are discussed, as they are of the utmost importance amid the current pandemic.
Dans l'actuelle pandémie de la COVID-19, le coronavirus du syndrome respiratoire aigu sévère 2 (SRAS-CoV-2) utilise les récepteurs de l'enzyme de conversion de l'angiotensine 2 (ECA-2) pour entrer dans les cellules, s'ensuit le dysfonctionnement et la régulation à la baisse de l'ECA-2, qui perturbent l’équilibre entre le système rénine-angiotensine (SRA) traditionnel et le SRA contre-régulateur en faveur du SRA traditionnel. La dysrégulation du SRA est l'une des caractéristiques principales des maladies cardiovasculaires. Par conséquent, l'ajustement de ce système est l'objectif thérapeutique principal. Les inhibiteurs du SRA, particulièrement les inhibiteurs de l'ECA (IECA) et les antagonistes des récepteurs de type 1 de l'angiotensine II (ARA), sont communément utilisés pour traiter l'hypertension et les maladies cardiovasculaires. Les patients atteints de maladies cardiovasculaires représentent le groupe le plus fréquemment observé parmi les patients atteints de comorbidités associées à la COVID-19. Au début de la pandémie, un dilemme à propos de l'utilisation des IECA et des ARA s'est posé, puisqu'ils aggravaient potentiellement la dysfonction cardiovasculaire et pulmonaire chez les patients atteints de la COVID-19. Des essais cliniques urgents issus de différents pays et hôpitaux ont montré qu'il n'y avait pas d'association entre le traitement par inhibiteurs du SRA et les complications liées à l'infection par la COVID-19 ou aux comorbidités. Néanmoins, la perturbation du SRA qui est associée à l'infection par la COVID-19 et le traitement potentiel dans ce champ restent à résoudre. Dans la présente revue, le lien entre la dysrégulation du SRA traditionnel et les activités contre-régulatrices du SRA chez les patients atteints de la COVID-19 qui ont des maladies cardiovasculaires métaboliques est étudié. De plus, nous nous penchons sur les plus récentes conclusions fondées sur l'administration des IECA et des ARA et la disponibilité de l'ECA2 en relation avec la COVID-19 pour offrir une meilleure compréhension de la contribution du SRA à la pathologie de la COVID-19, puisqu'ils sont de la plus haute importance dans le contexte de l'actuelle pandémie.
© 2021 The Authors.
Figures
References
-
- Fernández-Ruiz I. Immune system and cardiovascular disease. Nat Rev Cardiol. 2016;13:503. - PubMed
-
- Barhoumi T, Kasal DA, Li MW. T regulatory lymphocytes prevent angiotensin II-induced hypertension and vascular injury. Hypertension. 2011;57:469–476. - PubMed
-
- Javeshghani D, Barhoumi T, Idris-Khodja N, Paradis P, Schiffrin EL. Reduced macrophage-dependent inflammation improves endothelin-1-induced vascular injury. Hypertension. 2013;62:112–117. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
