

Does Maintenance of Pulmonary Blood Flow Pulsatility at the Time of the Fontan Operation Improve Hemodynamic Outcome in Functionally Univentricular Hearts?
- PMID: 33876263
- PMCID: PMC8192359
- DOI: 10.1007/s00246-021-02599-w
Does Maintenance of Pulmonary Blood Flow Pulsatility at the Time of the Fontan Operation Improve Hemodynamic Outcome in Functionally Univentricular Hearts?
Abstract
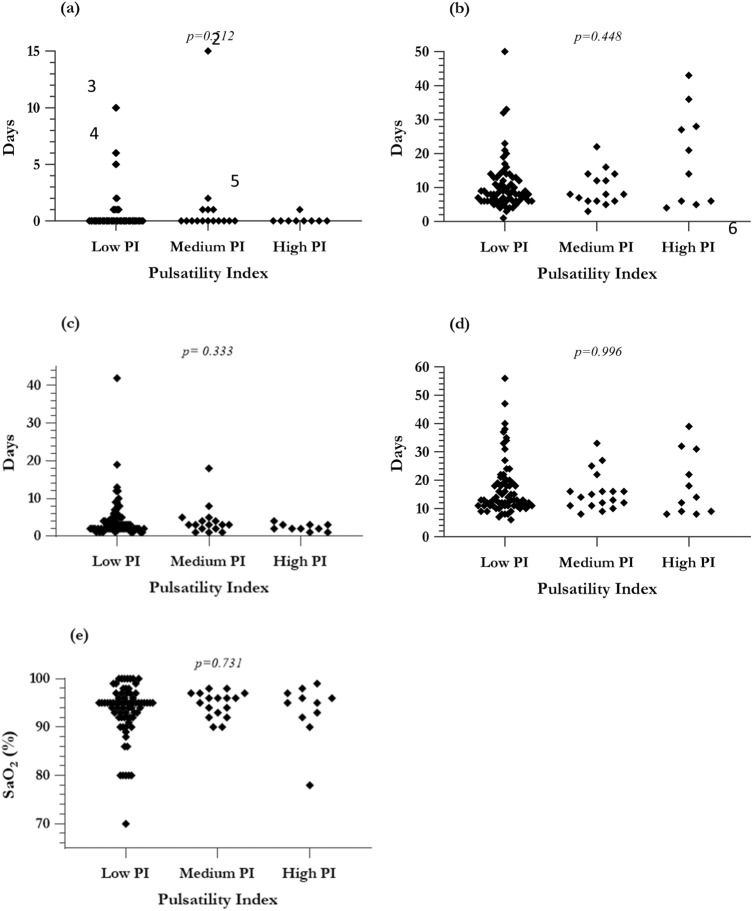
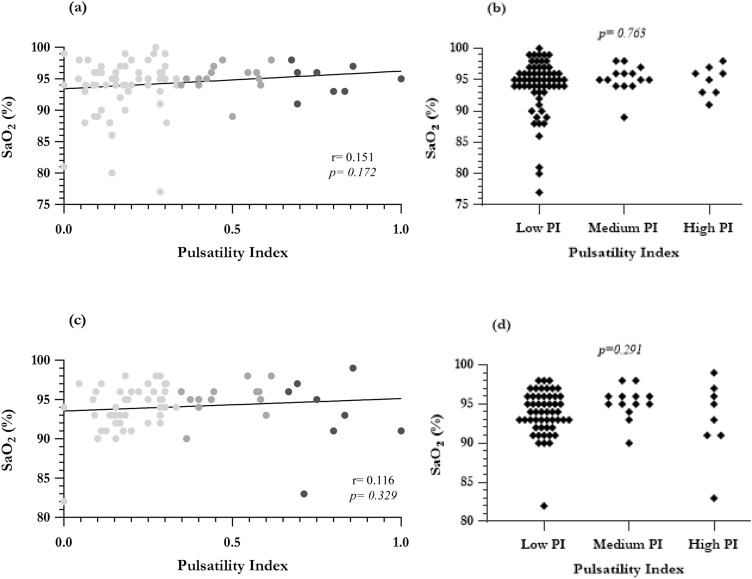
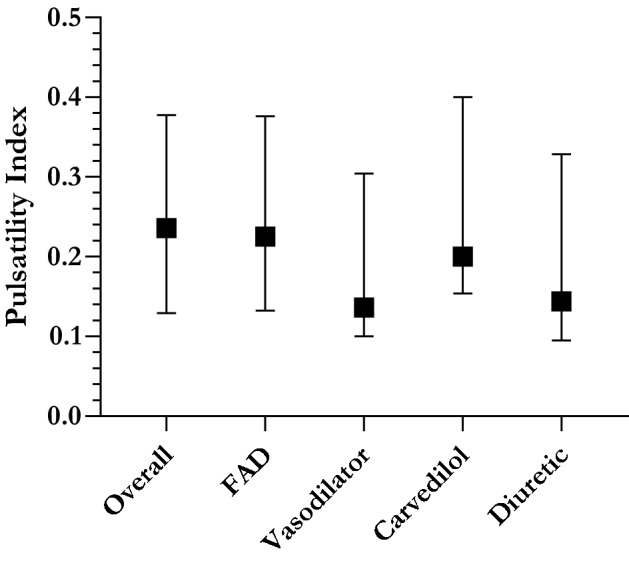
It is unclear whether residual anterograde pulmonary blood flow (APBF) at the time of Fontan is beneficial. Pulsatile pulmonary flow may be important in maintaining a compliant and healthy vascular circuit. We, therefore, wished to ascertain whether there was hemodynamic evidence that residual pulsatile flow at time of Fontan promotes clinical benefit. 106 consecutive children with Fontan completion (1999-2018) were included. Pulmonary artery pulsatility index (PI, (systolic pressure-diastolic pressure)/mean pressure)) was calculated from preoperative cardiac catheterization. Spectral analysis charted PI as a continuum against clinical outcome. The population was subsequently divided into three pulsatility subgroups to facilitate further comparison. Median PI prior to Fontan was 0.236 (range 0-1). 39 had APBF, in whom PI was significantly greater (median: 0.364 vs. 0.177, Mann-Whitney p < 0.0001). There were four early hospital deaths (3.77%), and PI in these patients ranged from 0.214 to 0.423. There was no correlation between PI and standard cardiac surgical outcomes or systemic oxygen saturation at discharge. Median follow-up time was 4.33 years (range 0.0273-19.6), with no late deaths. Increased pulsatility was associated with higher oxygen saturations in the long term, but there was no difference in reported exercise tolerance (Ross), ventricular function, or atrioventricular valve regurgitation at follow-up. PI in those with Fontan-associated complications or the requiring pulmonary vasodilators aligned with the overall population median. Maintenance of pulmonary flow pulsatility did not alter short-term outcomes or long-term prognosis following Fontan although it tended to increase postoperative oxygen saturations, which may be beneficial in later life.
Keywords: Congenital heart surgery; Fontan; Pulmonary vascular resistance.
Conflict of interest statement
The authors have no relevant affiliations or financial involvement with any commercial organization with a financial interest in or financial conflict with the subject matter discussed in the manuscript. No writing assistance was sought to produce this manuscript.
Figures
Similar articles
-
Bidirectional cavopulmonary shunt with additional pulmonary blood flow: a failed or successful strategy?Eur J Cardiothorac Surg. 2012 Sep;42(3):513-9. doi: 10.1093/ejcts/ezs053. Epub 2012 Feb 24. Eur J Cardiothorac Surg. 2012. PMID: 22368190
-
Significance of additional pulmonary blood flow between second and third stage in Fontan pathway.BMC Pediatr. 2024 Nov 6;24(1):705. doi: 10.1186/s12887-024-05183-2. BMC Pediatr. 2024. PMID: 39506657 Free PMC article.
-
The effect of antegrade pulmonary blood flow following a late bidirectional Glenn procedure.Interact Cardiovasc Thorac Surg. 2018 Mar 1;26(3):454-459. doi: 10.1093/icvts/ivx325. Interact Cardiovasc Thorac Surg. 2018. PMID: 29049710
-
Impact of Pulsatile Bidirectional Cavopulmonary Shunt on Pre-Fontan Hemodynamics in Single Ventricle Physiology: A Meta-Analysis Reveals Favorable Outcomes.Ann Thorac Cardiovasc Surg. 2025;31(1):24-00170. doi: 10.5761/atcs.ra.24-00170. Ann Thorac Cardiovasc Surg. 2025. PMID: 40010718 Free PMC article.
-
Extracardiac Fontan operation without cardiopulmonary bypass.J Cardiovasc Surg (Torino). 2006 Dec;47(6):699-704. J Cardiovasc Surg (Torino). 2006. PMID: 17043618 Review.
Cited by
-
Evaluation of Pulmonary Blood Flow Pulsatility in Patients Undergoing Various Fontan Palliation Techniques.J Cardiovasc Imaging. 2022 Apr;30(2):109-111. doi: 10.4250/jcvi.2021.0180. J Cardiovasc Imaging. 2022. PMID: 35505499 Free PMC article. No abstract available.
-
Unique Pulmonary Hypertensive Vascular Diseases Associated with Heart and Lung Developmental Defects.J Cardiovasc Dev Dis. 2023 Aug 3;10(8):333. doi: 10.3390/jcdd10080333. J Cardiovasc Dev Dis. 2023. PMID: 37623346 Free PMC article. Review.
References
-
- Baumgartner H, Bonhoeffer P, De Groot NM, de Haan F, Deanfield JE, Galie N, et al. ESC Guidelines for the management of grown-up congenital heart disease (new version 2010) Eur Heart J. 2010;31(23):2915–2957. - PubMed
-
- O'Leary PW. Prevalence, clinical presentation and natural history of patients with single ventricle. Prog Pediatr Cardiol. 2002;16(1):31–38.
-
- d'Udekem Y, Iyengar AJ, Cochrane AD, Grigg LE, Ramsay JM, Wheaton GR, et al. The Fontan procedure: contemporary techniques have improved long-term outcomes. Circulation. 2007;116(11 Suppl):I157–I164. - PubMed
-
- Tweddell JS, Nersesian M, Mussatto KA, Nugent M, Simpson P, Mitchell ME, et al. Fontan palliation in the modern era: factors impacting mortality and morbidity. Ann Thorac Surg. 2009;88(4):1291–1299. - PubMed
-
- Dabal RJ, Kirklin JK, Kukreja M, Brown RN, Cleveland DC, Eddins MC, et al. The modern Fontan operation shows no increase in mortality out to 20 years: a new paradigm. J Thorac Cardiovasc Surg. 2014;148(6):2517–23.e1. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
