

Chronic use of renin-angiotensin-aldosterone system blockers and mortality in COVID-19: A multicenter prospective cohort and literature review
- PMID: 33876439
- PMCID: PMC8250758
- DOI: 10.1111/fcp.12683
Chronic use of renin-angiotensin-aldosterone system blockers and mortality in COVID-19: A multicenter prospective cohort and literature review
Abstract
Aims: The role of renin-angiotensin-aldosterone system (RAAS) blockers on the course of coronavirus disease 2019 (COVID-19) is debated. We assessed the association between chronic use of RAAS blockers and mortality among inpatients with COVID-19 and explored reasons for discrepancies in the literature.
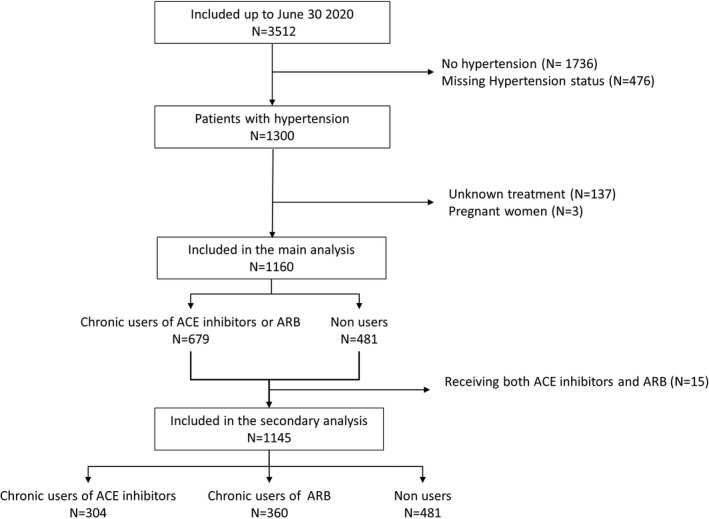
Methods and results: We included adult hypertensive patients from a prospective nationwide cohort of 3512 inpatients with COVID-19 up to June 30, 2020. Cox proportional hazard models with various adjustment or propensity weighting methods were used to estimate the hazard ratios (HR) of 30-day mortality for chronic users versus non-users of RAAS blockers. We analyzed data of 1160 hypertensive patients: 719 (62%) were male and 777 (67%) were older than 65 years. The main comorbidities were diabetes (n = 416, 36%), chronic cardiac disease (n = 401, 35%), and obesity (n = 340, 29%); 705 (61%) received oxygen therapy. We recorded 135 (11.6%) deaths within 30 days of diagnosis. We found no association between chronic use of RAAS blockers and mortality (unadjusted HR = 1.13, 95% CI [0.8-1.6]; propensity inverse probability treatment weighted HR = 1.09 [0.86-1.39]; propensity standardized mortality ratio weighted HR = 1.08 [0.79-1.47]). Our comprehensive review of previous studies highlighted that significant associations were mostly found in unrestricted populations with inappropriate adjustment, or with biased in-hospital exposure measurement.
Conclusion: Our results do not support previous concerns regarding these drugs, nor a potential protective effect as reported in previous poorly designed studies and meta-analyses. RAAS blockers should not be discontinued during the pandemic, while in-hospital management of these drugs will be clarified by randomized trials. NCT04262921.
Keywords: COVID-19; RAAS blockers; angiotensin antagonists; hypertension; mortality; propensity score.
© 2021 Société Française de Pharmacologie et de Thérapeutique.
Conflict of interest statement
MR received travel funding from Pfizer, outside the submitted work. APHP, which employs JSH, has received research grants from Bioserenity, Sanofi, Servier, and Novo Nordisk. JSH received speaker, advisory board, or consultancy fees from Amgen, Astra Zeneca, Bayer, Bristol‐Myers Squibb, Novartis, Novo Nordisk, WeHealth, outside the submitted work. BL reports travel funding from ViiV (2019) and Gilead (2020), outside the submitted work. PR reports personal fees (consulting) from Idorsia and G3P and honoraria from AstraZeneca, Bayer, Boehringer Ingelheim, CVRx, Fresenius, Grunenthal, Novartis, Novo Nordisk, Sequana medical, Servier, Stealth Peptides, Ablative Solutions, Corvidia, Relypsa, Vifor, and Vifor Fresenius Medical Care Renal Pharma; outside the submitted work. PR is the cofounder of CardioRenal (outside the submitted work). DC reports HIV grants from Janssen (2017‐2018, 2019‐2020) and MSD France (2015‐2017), personal fees from Janssen (2018), MSD France (2017) and Gilead (2018, 2020) for lectures on HIV, and personal fees from Merck Switzerland (2017) for consultancy on multiple sclerosis, outside the submitted work. EVP received fees and travel funding from Servier, outside the submitted work.
Figures
References
-
- Wu Z, McGoogan JM. Characteristics of and important lessons from the coronavirus disease 2019 (COVID‐19) outbreak in China: summary of a report of 72 314 cases from the Chinese Center for Disease Control and Prevention. JAMA. 2020;323:1239–1242. - PubMed
-
- Ferrario CM, Jessup J, Chappell MC et al. Effect of angiotensin‐converting enzyme inhibition and angiotensin II receptor blockers on cardiac angiotensin‐converting enzyme 2. Circulation. 2005;111:2605–2610. - PubMed
-
- Soler MJ, Ye M, Wysocki J, William J, Lloveras J, Batlle D. Localization of ACE2 in the renal vasculature: amplification by angiotensin II type 1 receptor blockade using telmisartan. Am J Physiol Renal Physiol. 2009;296:F398–F405. - PubMed
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
