

Gut Microbiome in Progressive Multiple Sclerosis
- PMID: 33876477
- PMCID: PMC8132291
- DOI: 10.1002/ana.26084
Gut Microbiome in Progressive Multiple Sclerosis
Abstract
Objective: This study was undertaken to investigate the gut microbiome in progressive multiple sclerosis (MS) and how it relates to clinical disease.
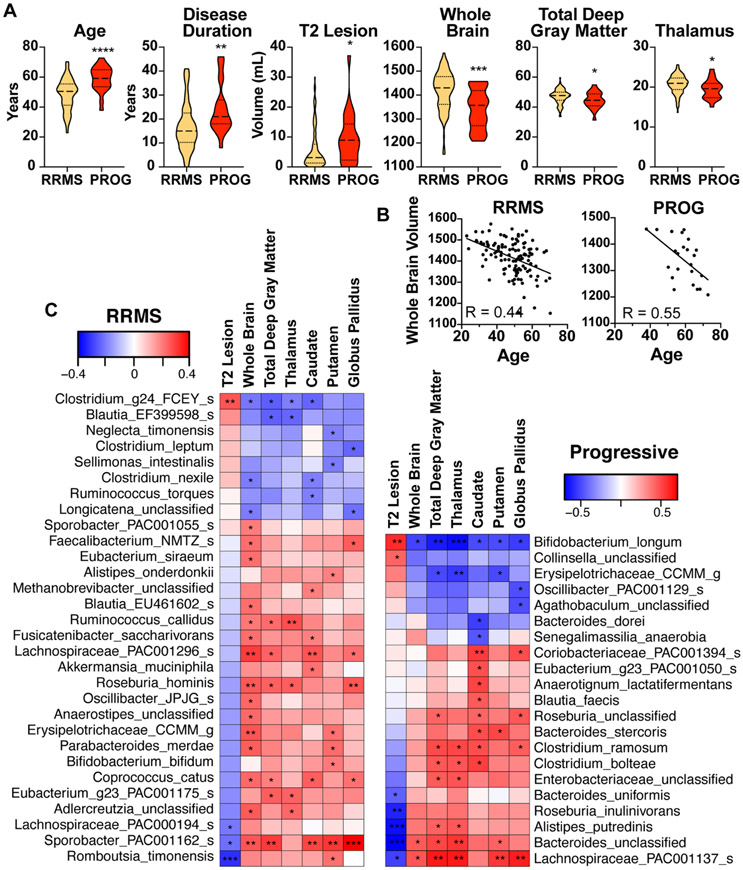
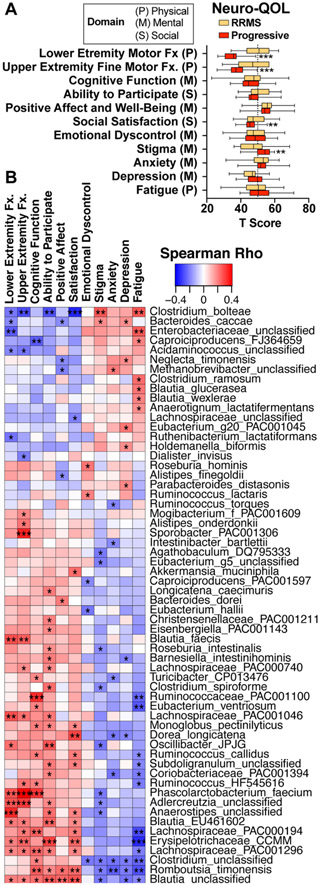
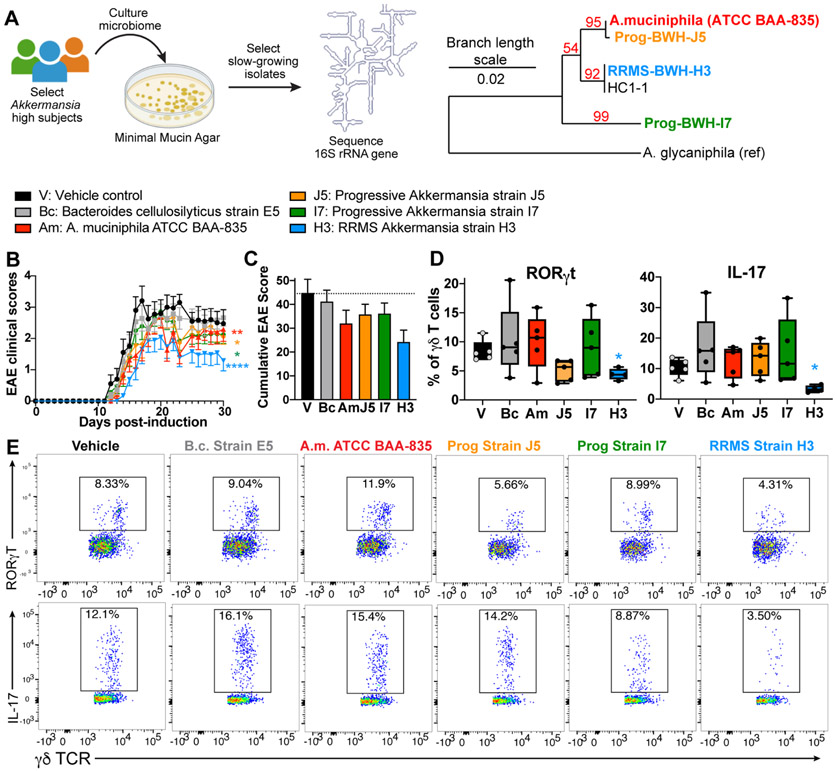
Methods: We sequenced the microbiota from healthy controls and relapsing-remitting MS (RRMS) and progressive MS patients and correlated the levels of bacteria with clinical features of disease, including Expanded Disability Status Scale (EDSS), quality of life, and brain magnetic resonance imaging lesions/atrophy. We colonized mice with MS-derived Akkermansia and induced experimental autoimmune encephalomyelitis (EAE).
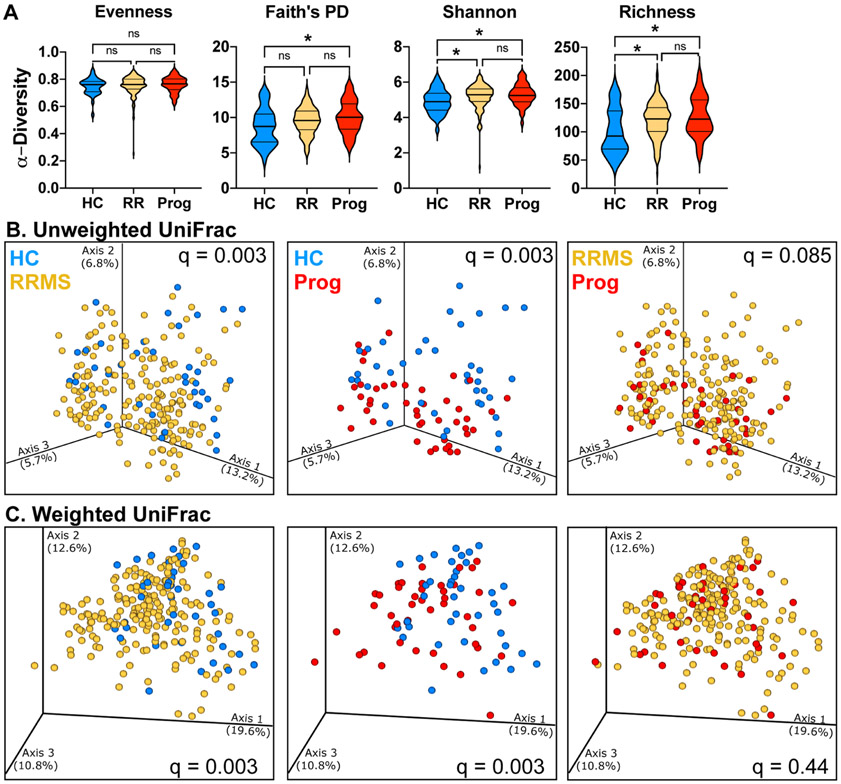
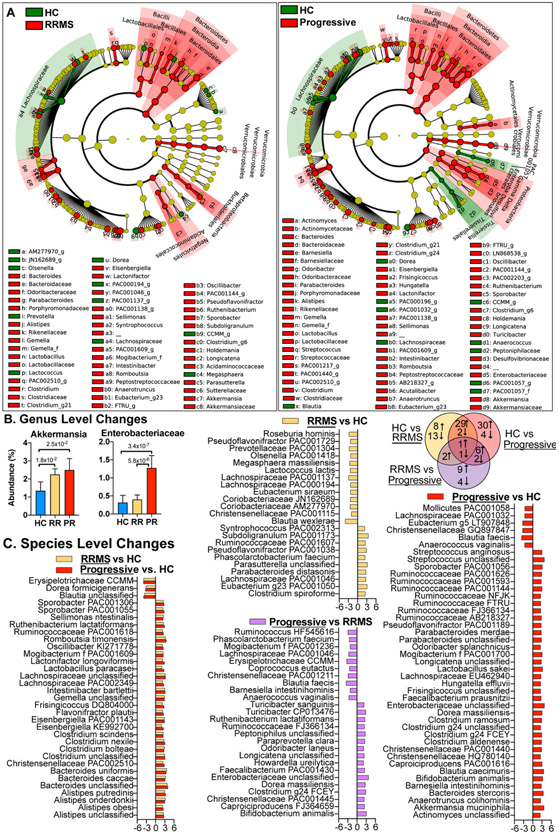
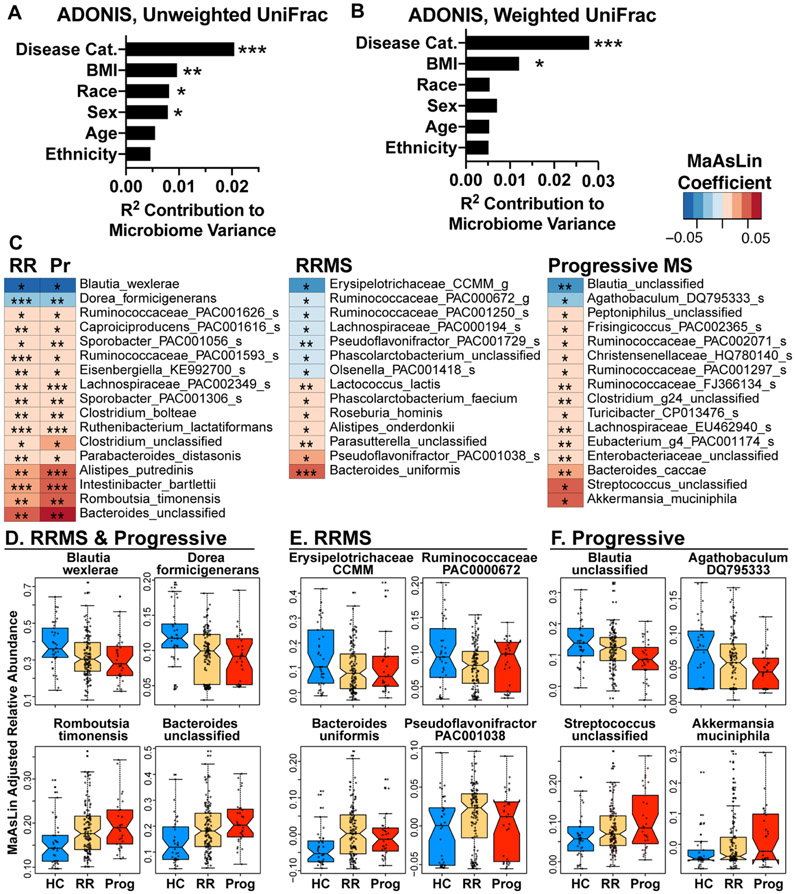
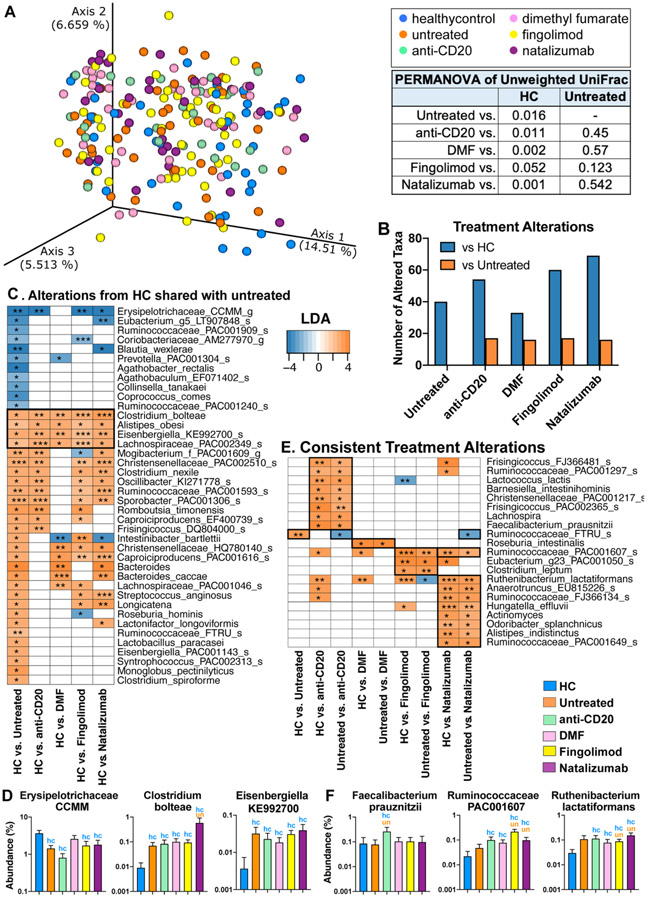
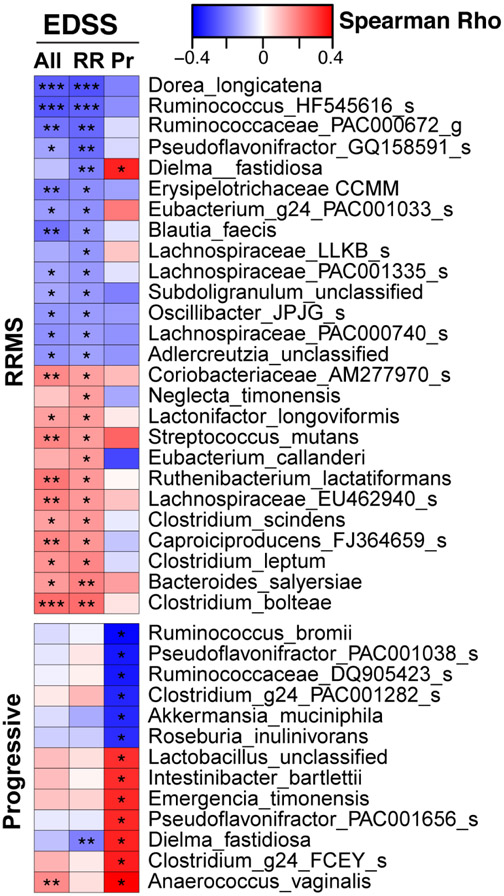
Results: Microbiota β-diversity differed between MS patients and controls but did not differ between RRMS and progressive MS or differ based on disease-modifying therapies. Disease status had the greatest effect on the microbiome β-diversity, followed by body mass index, race, and sex. In both progressive MS and RRMS, we found increased Clostridium bolteae, Ruthenibacterium lactatiformans, and Akkermansia and decreased Blautia wexlerae, Dorea formicigenerans, and Erysipelotrichaceae CCMM. Unique to progressive MS, we found elevated Enterobacteriaceae and Clostridium g24 FCEY and decreased Blautia and Agathobaculum. Several Clostridium species were associated with higher EDSS and fatigue scores. Contrary to the view that elevated Akkermansia in MS has a detrimental role, we found that Akkermansia was linked to lower disability, suggesting a beneficial role. Consistent with this, we found that Akkermansia isolated from MS patients ameliorated EAE, which was linked to a reduction in RORγt+ and IL-17-producing γδ T cells.
Interpretation: Whereas some microbiota alterations are shared in relapsing and progressive MS, we identified unique bacteria associated with progressive MS and clinical measures of disease. Furthermore, elevated Akkermansia in MS may be a compensatory beneficial response in the MS microbiome. ANN NEUROL 2021;89:1195-1211.
© 2021 American Neurological Association.
Conflict of interest statement
POTENTIAL CONFLICTS OF INTEREST
Nothing to report.
Figures
References
-
- Lee YK, Menezes JS, Umesaki Y, Mazmanian SK. Proinflammatory T-cell responses to gut microbiota promote experimental autoimmune encephalomyelitis. Proc Natl Acad Sci U S A. 2011;108 Suppl 1 (Supplement 1):4615–22. Epub 2010/07/28. doi: 10.1073/pnas.1000082107. PubMed PMID: 20660719; PMCID: PMC3063590. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
