

Diffusion-weighted imaging in differentiating mid-course responders to chemotherapy for long-bone osteosarcoma compared to the histologic response: an update
- PMID: 33877417
- PMCID: PMC8363524
- DOI: 10.1007/s00247-021-05037-4
Diffusion-weighted imaging in differentiating mid-course responders to chemotherapy for long-bone osteosarcoma compared to the histologic response: an update
Abstract
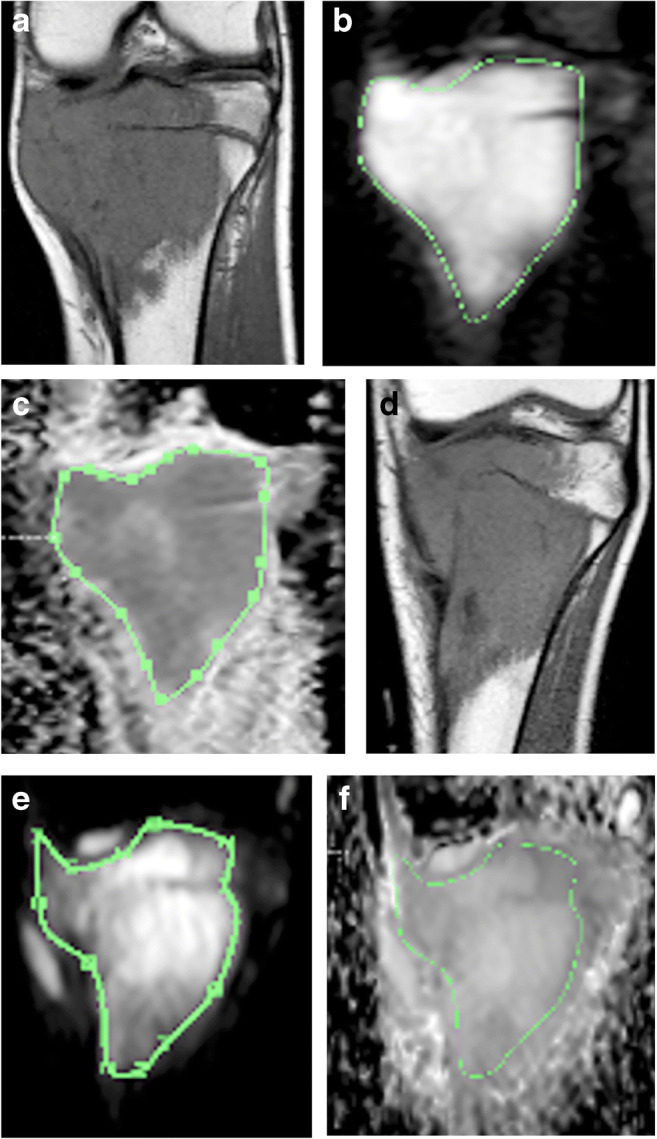
Background: Diffusion-weighted imaging (DWI) has been described to correlate with tumoural necrosis in response to preoperative chemotherapy for osteosarcoma.
Objective: To assess the accuracy of DWI in evaluating the response to neoadjuvant chemotherapy at the mid-course treatment of long-bone osteosarcoma and in predicting survival.
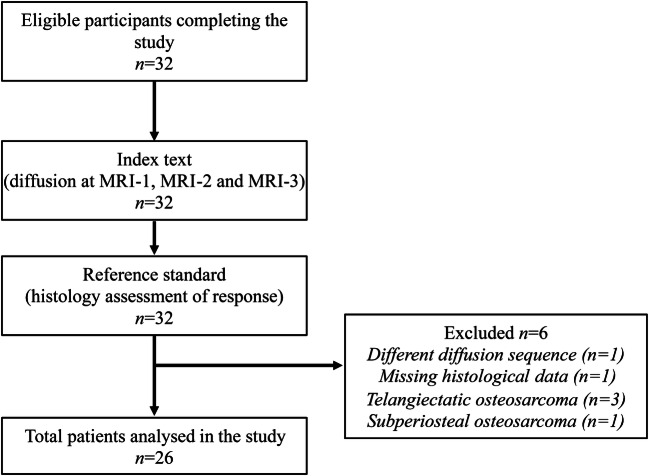
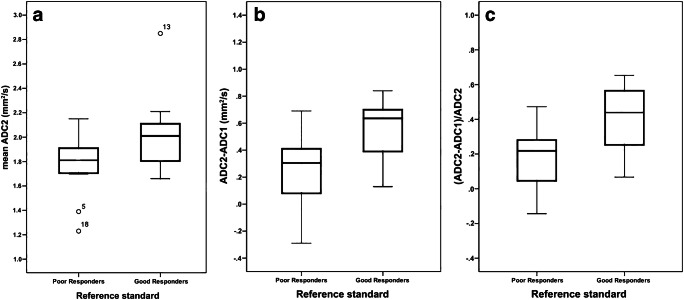
Materials and methods: We conducted a prospective single-centre study over a continuous period of 11 years. Consecutive patients younger than 20 years treated with a neoadjuvant regimen for peripheral conventional osteosarcoma were eligible for inclusion. Magnetic resonance imaging (MRI) with DWI was performed at diagnosis, and mid- and end-course chemotherapy with mean apparent diffusion coefficients (ADC) calculated at each time point. A percentage less than or equal to 10% of the viable residual tissue at the histological analysis of the surgical specimen was defined as a good responder to chemotherapy. Survival comparisons were calculated using the Kaplan-Meier method. Uni- and multivariate analyses with ADC change were performed by Cox modelling. This is an expansion and update of our previous work.
Results: Twenty-six patients between the ages of 4.8 and 19.6 years were included, of whom 14 were good responders. At mid-course chemotherapy, good responders had significantly higher mean ADC values (P=0.046) and a higher increase in ADC (P=0.015) than poor responders. The ADC change from diagnosis to mid-course MRI did not appear to be a prognosticator of survival and did not impact survival rates of both groups.
Conclusion: DWI at mid-course preoperative chemotherapy for osteosarcoma should be considered to evaluate the degree of histological necrosis and to predict survival. The anticipation of a response to neoadjuvant treatment by DWI may have potential implications on preoperative management.
Keywords: Bone neoplasm; Children; Diffusion-weighted imaging; Magnetic resonance imaging; Osteosarcoma; Therapeutic response.
© 2021. The Author(s).
Conflict of interest statement
None
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
