

National Institutes of Health Consensus Development Project on Criteria for Clinical Trials in Chronic Graft-versus-Host Disease: I. The 2020 Etiology and Prevention Working Group Report
- PMID: 33877965
- PMCID: PMC8217141
- DOI: 10.1016/j.jtct.2021.02.035
National Institutes of Health Consensus Development Project on Criteria for Clinical Trials in Chronic Graft-versus-Host Disease: I. The 2020 Etiology and Prevention Working Group Report
Abstract
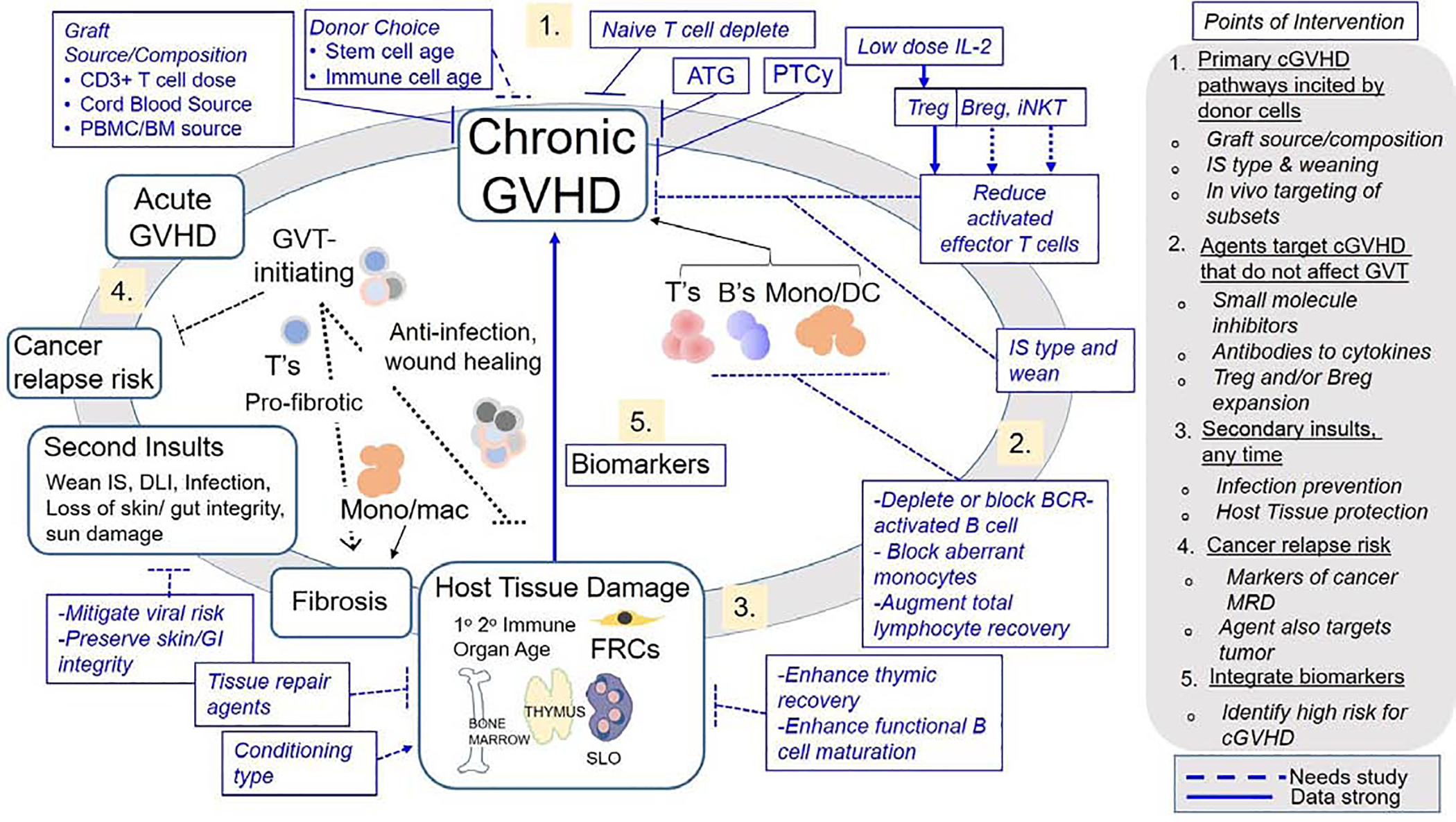
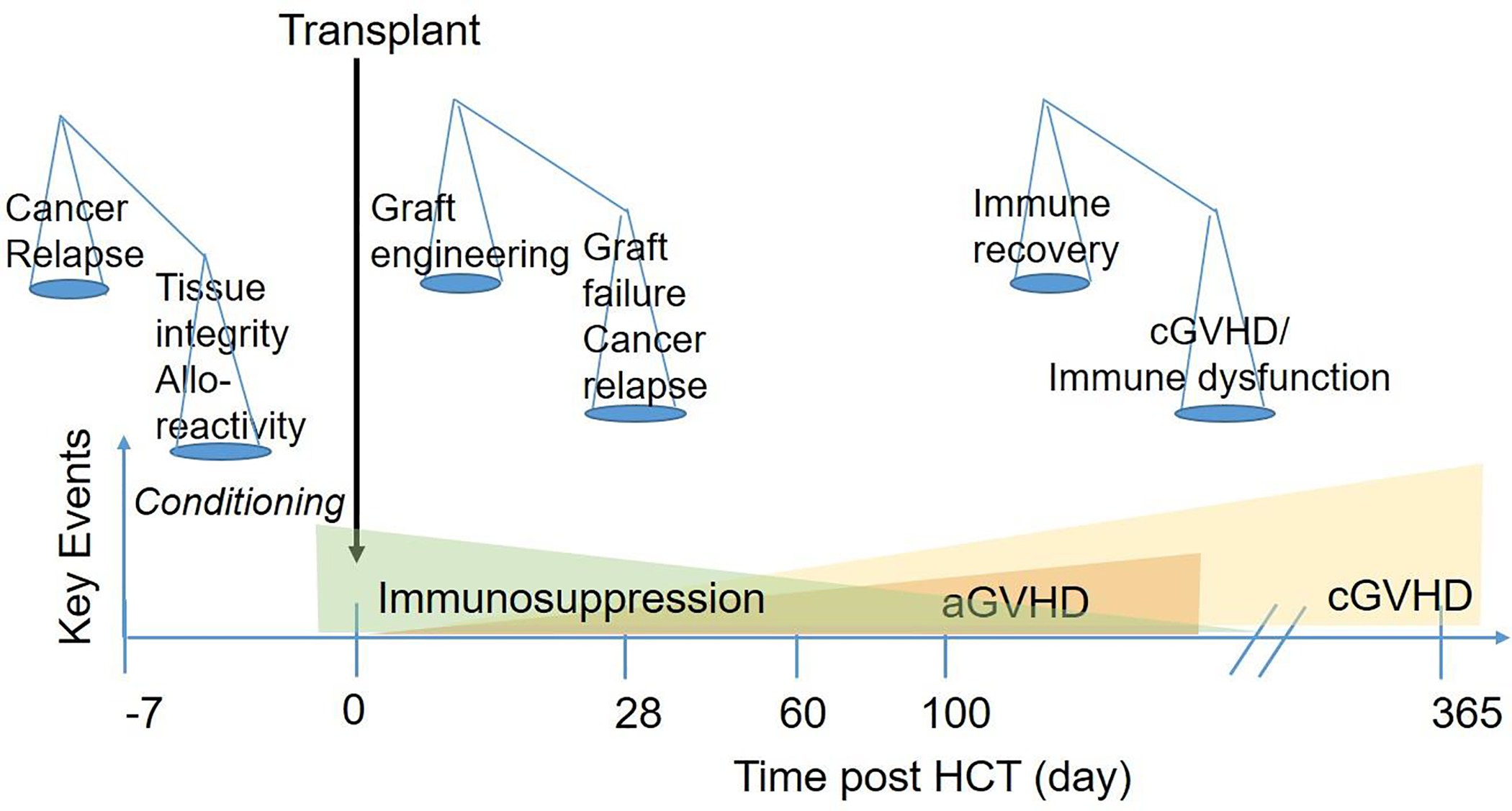
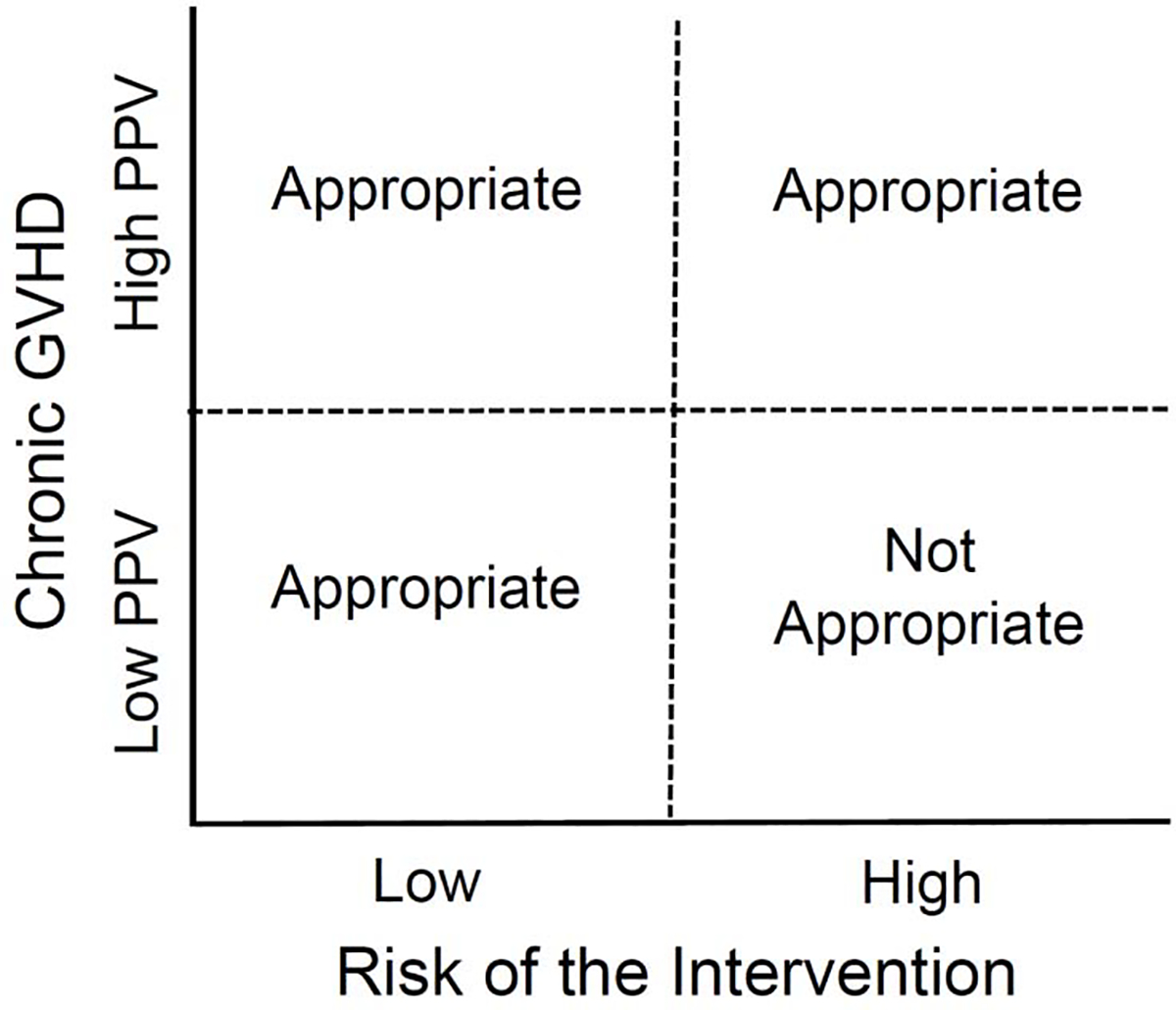
Preventing chronic graft-versus-host disease (GVHD) remains challenging because the unique cellular and molecular pathways that incite chronic GVHD are poorly understood. One major point of intervention for potential prevention of chronic GVHD occurs at the time of transplantation when acute donor anti-recipient immune responses first set the events in motion that result in chronic GVHD. After transplantation, additional insults causing tissue injury can incite aberrant immune responses and loss of tolerance, further contributing to chronic GVHD. Points of intervention are actively being identified so that chronic GVHD initiation pathways can be targeted without affecting immune function. The major objective in the field is to continue basic studies and to translate what is learned about etiopathology to develop targeted prevention strategies that decrease the risk of morbid chronic GVHD without increasing the risks of cancer relapse or infection. Development of strategies to predict the risk of developing debilitating or deadly chronic GVHD is a high research priority. This working group recommends further interrogation into the mechanisms underpinning chronic GVHD development, and we highlight considerations for future trial design in prevention trials.
Copyright © 2021 The American Society for Transplantation and Cellular Therapy. All rights reserved.
Conflict of interest statement
Financial disclosure:
Figures
References
-
- Cooke KR, Luznik L, Sarantopoulos S, Hakim FT, Jagasia M, Fowler DH, et al. The Biology of Chrnic Graft-versus-Host Disease: A Task Force Report from the National Institutes of Health Consensus Development Project on Criteria for Clinical Trials in Chronic Graft-versus-Host Disease. Biol Blood Marrow Transplant. 2017;23:211–34. - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
