

Early ultrasound evaluation identifies excellent responders to neoadjuvant systemic therapy among patients with triple-negative breast cancer
- PMID: 33878210
- PMCID: PMC8319084
- DOI: 10.1002/cncr.33604
Early ultrasound evaluation identifies excellent responders to neoadjuvant systemic therapy among patients with triple-negative breast cancer
Abstract
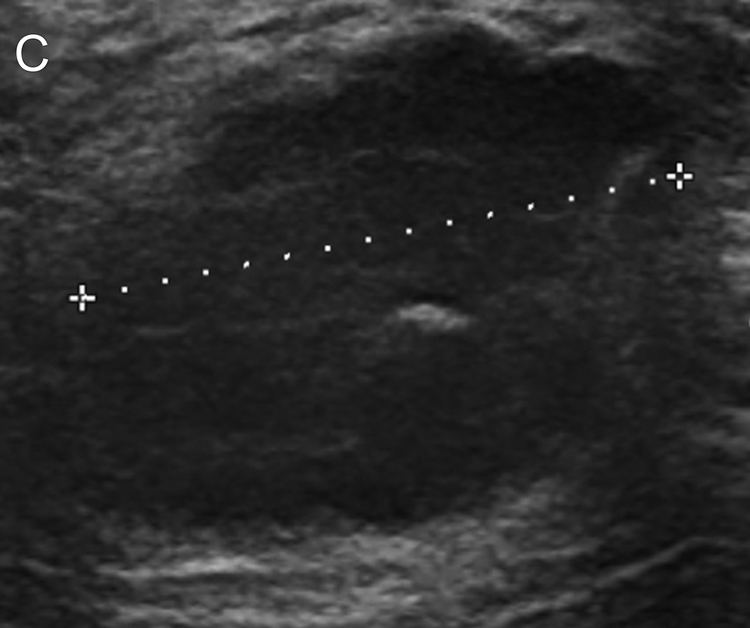
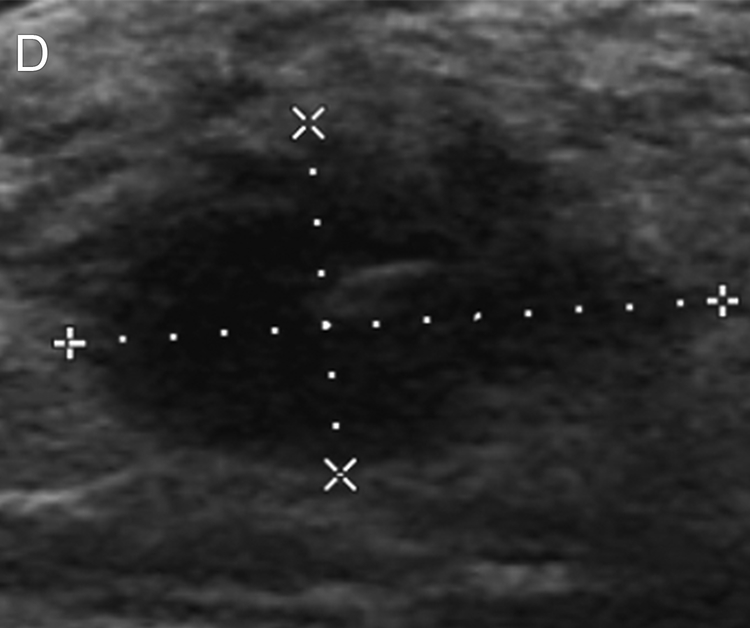
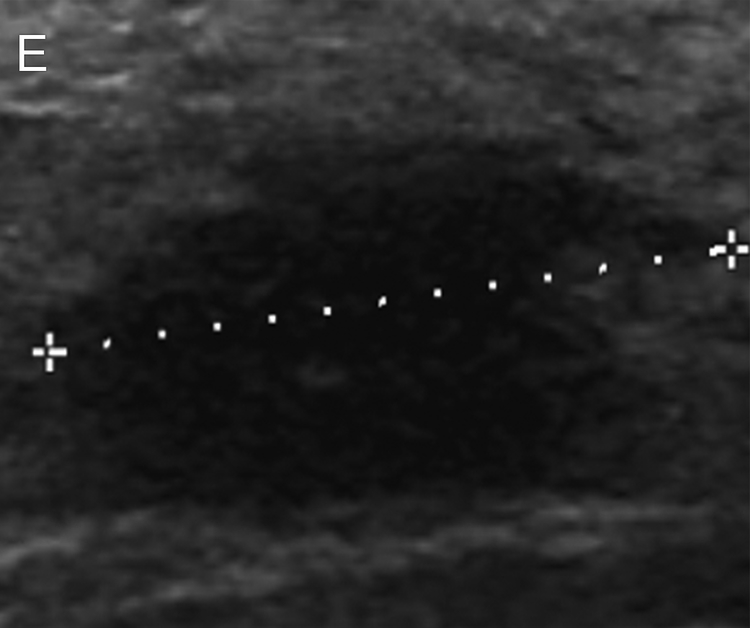
Background: Heterogeneity exists in the response of triple-negative breast cancer (TNBC) to standard anthracycline (AC)/taxane-based neoadjuvant systemic therapy (NAST), with 40% to 50% of patients having a pathologic complete response (pCR) to therapy. Early assessment of the imaging response during NAST may identify a subset of TNBCs that are likely to have a pCR upon completion of treatment. The authors aimed to evaluate the performance of early ultrasound (US) after 2 cycles of neoadjuvant NAST in identifying excellent responders to NAST among patients with TNBC.
Methods: Two hundred fifteen patients with TNBC were enrolled in the ongoing ARTEMIS (A Robust TNBC Evaluation Framework to Improve Survival) clinical trial. The patients were divided into a discovery cohort (n = 107) and a validation cohort (n = 108). A receiver operating characteristic analysis with 95% confidence intervals (CIs) and a multivariate logistic regression analysis were performed to model the probability of a pCR on the basis of the tumor volume reduction (TVR) percentage by US from the baseline to after 2 cycles of AC.
Results: Overall, 39.3% of the patients (42 of 107) achieved a pCR. A positive predictive value (PPV) analysis identified a cutoff point of 80% TVR after 2 cycles; the pCR rate was 77% (17 of 22) in patients with a TVR ≥ 80%, and the area under the curve (AUC) was 0.84 (95% CI, 0.77-0.92; P < .0001). In the validation cohort, the pCR rate was 44%. The PPV for pCR with a TVR ≥ 80% after 2 cycles was 76% (95% CI, 55%-91%), and the AUC was 0.79 (95% CI, 0.70-0.87; P < .0001).
Conclusions: The TVR percentage by US evaluation after 2 cycles of NAST may be a cost-effective early imaging biomarker for a pCR to AC/taxane-based NAST.
Keywords: breast cancer; imaging; neoadjuvant systemic therapy (NAST); triple-negative breast cancer (TNBC); ultrasound.
© 2021 American Cancer Society.
Figures





Similar articles
-
MRI-Based Digital Models Forecast Patient-Specific Treatment Responses to Neoadjuvant Chemotherapy in Triple-Negative Breast Cancer.Cancer Res. 2022 Sep 16;82(18):3394-3404. doi: 10.1158/0008-5472.CAN-22-1329. Cancer Res. 2022. PMID: 35914239 Free PMC article.
-
Quantitative Apparent Diffusion Coefficients From Peritumoral Regions as Early Predictors of Response to Neoadjuvant Systemic Therapy in Triple-Negative Breast Cancer.J Magn Reson Imaging. 2022 Dec;56(6):1901-1909. doi: 10.1002/jmri.28219. Epub 2022 May 2. J Magn Reson Imaging. 2022. PMID: 35499264 Free PMC article.
-
Diffusion Tensor Imaging for Characterizing Changes in Triple-Negative Breast Cancer During Neoadjuvant Systemic Therapy.J Magn Reson Imaging. 2024 Oct;60(4):1367-1376. doi: 10.1002/jmri.29267. Epub 2024 Jan 31. J Magn Reson Imaging. 2024. PMID: 38294179
-
Tumor necrosis by pretreatment breast MRI: association with neoadjuvant systemic therapy (NAST) response in triple-negative breast cancer (TNBC).Breast Cancer Res Treat. 2021 Jan;185(1):1-12. doi: 10.1007/s10549-020-05917-7. Epub 2020 Sep 13. Breast Cancer Res Treat. 2021. PMID: 32920733 Free PMC article. Review.
-
Neoadjuvant systemic therapy in geriatric breast cancer patients: a National Cancer Database (NCDB) analysis.Breast Cancer Res Treat. 2022 Dec;196(3):441-451. doi: 10.1007/s10549-022-06751-9. Epub 2022 Oct 8. Breast Cancer Res Treat. 2022. PMID: 36207620 Review.
Cited by
-
Prediction model for assessing HER2 status patient with invasive ductal carcinoma based on clinical parameters and ultrasound features: a dual-center study.BMC Womens Health. 2025 Jul 3;25(1):291. doi: 10.1186/s12905-025-03828-7. BMC Womens Health. 2025. PMID: 40611065 Free PMC article.
-
Value of Histogram of Gray-Scale Ultrasound Image in Differential Diagnosis of Small Triple Negative Breast Invasive Ductal Carcinoma and Fibroadenoma.Cancer Manag Res. 2022 Apr 21;14:1515-1524. doi: 10.2147/CMAR.S359986. eCollection 2022. Cancer Manag Res. 2022. PMID: 35478712 Free PMC article.
-
Correlation between Baseline Conventional Ultrasounds, Shear-Wave Elastography Indicators, and Neoadjuvant Therapy Efficacy in Triple-Negative Breast Cancer.Diagnostics (Basel). 2023 Oct 11;13(20):3178. doi: 10.3390/diagnostics13203178. Diagnostics (Basel). 2023. PMID: 37891999 Free PMC article.
-
Neoadjuvant chemotherapy for breast cancer: an evaluation of its efficacy and research progress.Front Oncol. 2023 Oct 3;13:1169010. doi: 10.3389/fonc.2023.1169010. eCollection 2023. Front Oncol. 2023. PMID: 37854685 Free PMC article. Review.
-
Predicting Pathological Complete Response in Breast Cancer After Two Cycles of Neoadjuvant Chemotherapy by Tumor Reduction Rate: A Retrospective Case-Control Study.J Breast Cancer. 2023 Apr;26(2):136-151. doi: 10.4048/jbc.2023.26.e12. Epub 2023 Mar 16. J Breast Cancer. 2023. PMID: 37051647 Free PMC article.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
