

Managing the risk of a COVID-19 outbreak from border arrivals
- PMID: 33878278
- PMCID: PMC8086931
- DOI: 10.1098/rsif.2021.0063
Managing the risk of a COVID-19 outbreak from border arrivals
Abstract
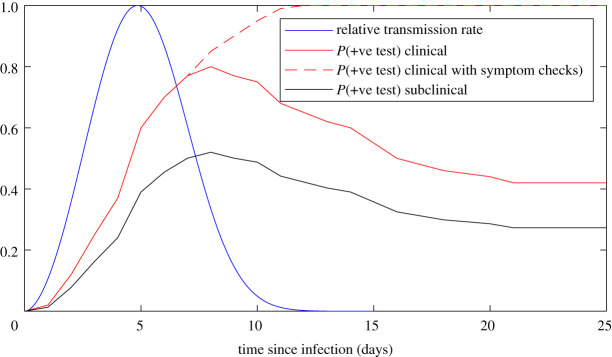
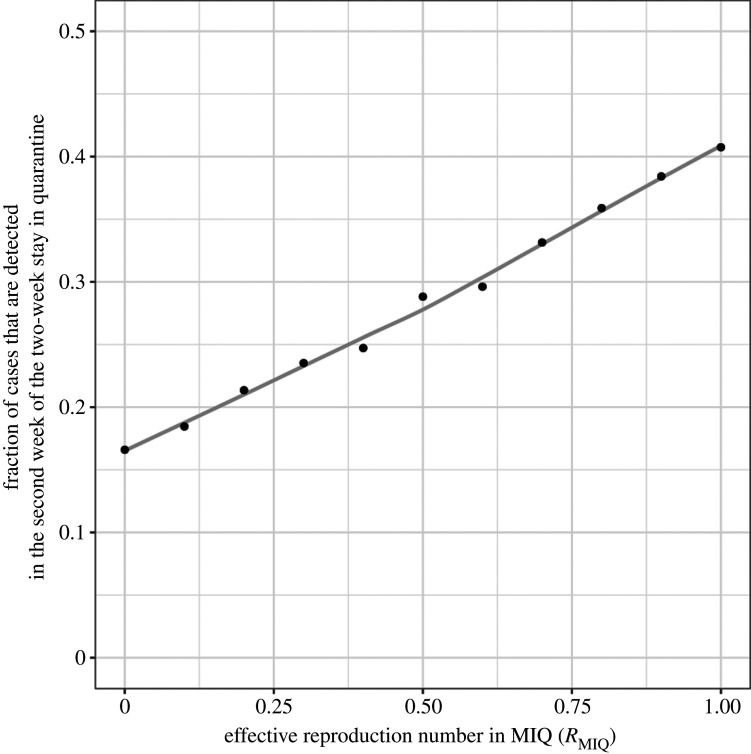
In an attempt to maintain the elimination of COVID-19 in New Zealand, all international arrivals are required to spend 14 days in government-managed quarantine and to return a negative test result before being released. We model the testing, isolation and transmission of COVID-19 within quarantine facilities to estimate the risk of community outbreaks being seeded at the border. We use a simple branching process model for COVID-19 transmission that includes a time-dependent probability of a false-negative test result. We show that the combination of 14-day quarantine with two tests is highly effective in preventing an infectious case entering the community, provided there is no transmission within quarantine facilities. Shorter quarantine periods, or reliance on testing only with no quarantine, substantially increases the risk of an infectious case being released. We calculate the fraction of cases detected in the second week of their two-week stay and show that this may be a useful indicator of the likelihood of transmission occurring within quarantine facilities. Frontline staff working at the border risk exposure to infected individuals and this has the potential to lead to a community outbreak. We use the model to test surveillance strategies and evaluate the likely size of the outbreak at the time it is first detected. We conclude with some recommendations for managing the risk of potential future outbreaks originating from the border.
Keywords: infectious disease outbreak; managed isolation and quarantine; stochastic model.
Figures





References
-
- World Health Organization. 2020. Coronavirus disease 2019 (COVID-19): situation report, 51. Geneva, Switzerland: World Health Organization.
-
- Clifford S, et al. . 2020. Strategies to reduce the risk of SARS-CoV-2 re-introduction from international travellers. medRxiv. (10.1101/2020.07.24.20161281) - DOI
-
- Golding N, et al. . 2020. Estimating temporal variation in transmission of SARS-CoV-2 and physical distancing behaviour in Australia. Melbourne, Australia: Doherty Institute.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical