

Rectal-vaginal pressure gradient in patients with pelvic organ prolapse and symptomatic rectocele
- PMID: 33879140
- PMCID: PMC8056717
- DOI: 10.1186/s12905-021-01304-6
Rectal-vaginal pressure gradient in patients with pelvic organ prolapse and symptomatic rectocele
Abstract
Objective: The aim of this study is to examine the relationship between rectal-vaginal pressure and symptomatic rectocele in patients with pelvic organ prolapse (POP).
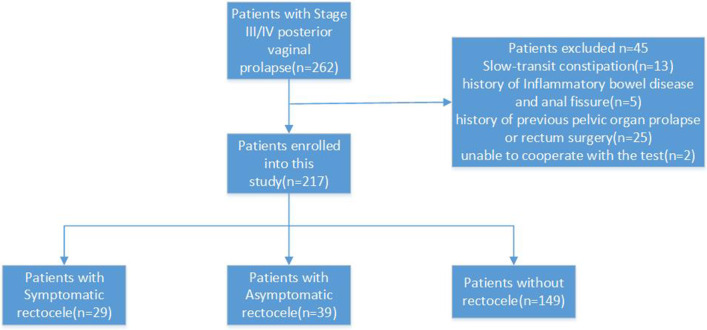
Method: Patients with posterior vaginal prolapse staged III or IV in accordance with the POP Quantitation classification method who were scheduled for pelvic floor reconstructive surgery in the years 2016-2019 were included in the study. Rectocele was diagnosed using translabial ultrasound, and obstructed defecation (OD) was diagnosed in accordance with the Roma IV diagnostic criteria. Both rectal and vaginal pressure were measured using peritron manometers at maximum Vasalva. To ensure stability, the test was performed three times with each patient.
Results: A total of 217 patients were enrolled in this study. True rectocele was diagnosed in 68 patients at a main rectal ampulla depth of 19 mm. Furthermore, 36 patients were diagnosed with OD. Symptomatic rectocele was significantly associated with older age (p < 0.01), a higher OD symptom score (p < 0.001), and a lower grade of apical prolapse (p < 0.001). The rectal-vaginal pressure gradient was higher in patients with symptomatic rectocele (37.4 ± 11.7 cm H2O) compared with patients with asymptomatic rectocele (16.9 ± 8.4 cm H2O, p < 0.001), and patients without rectocele (17.1 ± 9.2 cm H2O, p < 0.001).
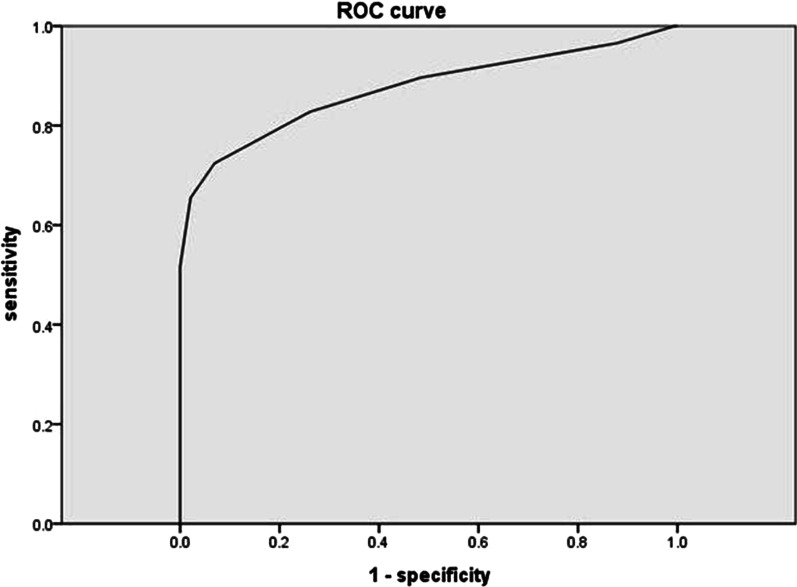
Conclusion: The rectal-vaginal pressure gradient was found to be a risk factor for symptomatic rectocele in patients with POP. A rectal-vaginal pressure gradient of > 27.5 cm H2O was suggested as the cut-off point of the elevated pressure gradient.
Keywords: Obstructed defecation; Pelvic organ prolapse; Rectal pressure; Rectocele; Vaginal pressure.
Conflict of interest statement
All of the authors had no any personal, financial, commercial, or academic conflicts of interest separately.
Figures

References
-
- Swift S. Classification and epidemiology of pelvic organ prolapse. Textbook of female urology and urogynecology, 3rd edn. 2010.
-
- Kenton K, Shott S, Brubaker L. The anatomic and functional variability of rectoceles in women. Int Urogynecol J. 1999;10(2):96–99. - PubMed
-
- Dietz HP, Steensma AB. Posterior compartment prolapse on two-dimensional and three-dimensional pelvic floor ultrasound: the distinction between true rectocele, perineal hypermobility and enterocele. Ultrasound Obstet Gynecol. 2005;26(1):73–77. - PubMed
-
- Shafik A, Mostafa RM, Shafik AA, El-Sibai O. Study of the effect of straining on the bulbocavernosus muscle with evidence of a straining–bulbocavernosus reflex and its clinical significance. Int Urogynecol J Pelvic Floor Dysfunct. 2002;13(5):294–298. - PubMed
-
- Shafik A. Straining puborectalis reflex: description and significance of a "new" reflex. Anat Rec. 1991;229(2):281–284. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
