

Surgical treatment of infective endocarditis in intravenous drug abusers
- PMID: 33879196
- PMCID: PMC8056573
- DOI: 10.1186/s13019-021-01491-1
Surgical treatment of infective endocarditis in intravenous drug abusers
Abstract
Background: Despite current progress in antibiotic therapy and medical management, infective endocarditis remains a serious condition presenting with high mortality rates. It also is a life-threatening complication in patients with a history of chronic intravenous drug abuse. In this study, we analyzed our institutional experience on the surgical therapy of infective endocarditis in patients with active intravenous drug abuse. The aim of the study is to identify the predictive factors of mortality and morbidity in this subgroup of patients.
Methods: Between 2007 and 2020, a total of 24 patients (7 female, mean age 38.5 ± 8.7) presenting with active intravenous drug abuse underwent a surgical treatment for the infective endocarditis at out center. The primary endpoint was survival at 30th day after the surgery. The secondary composite endpoint included freedom from death, recurrent endocarditis, re-do surgery, and postoperative stroke during the follow-up period. Mean follow-up was 4.2 ± 4.3 years.
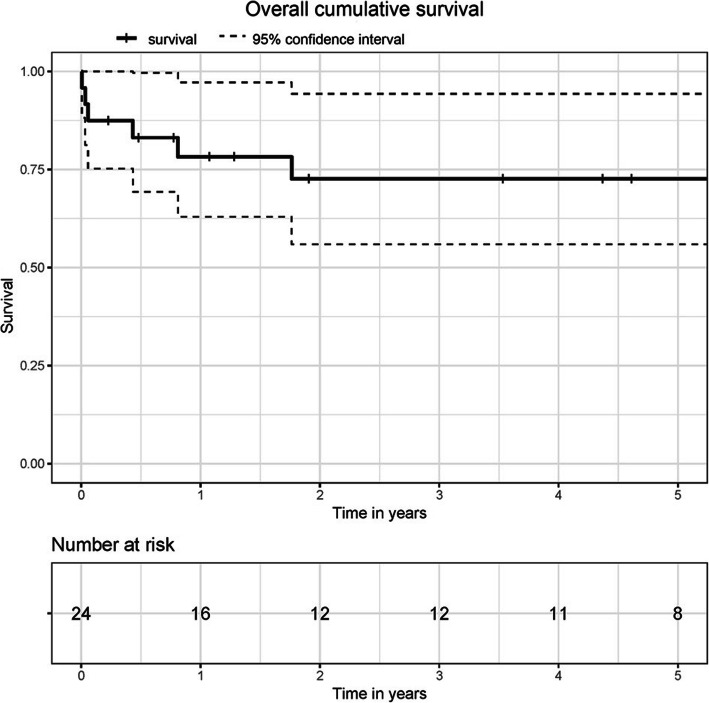
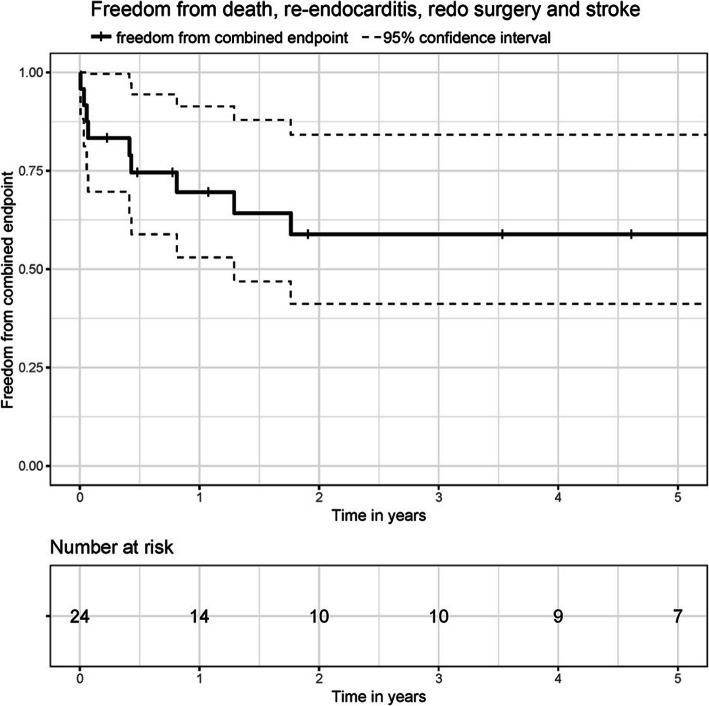
Results: Staphylococcus species was the most common pathogen detected in the preoperative blood cultures. Infection caused by Enterococcus species as well as liver function impairment were identified as mortality predictor factors. Logistic EuroSCORE and EusoSCORE-II were also predictive factors for mortality in univariate analysis. Survival at 1 and 3 years was 78 and 72% respectively. Thirty-day survival was 88%. 30-day freedom from combined endpoint was 83% and after 1 and 3 years, 69 and 58% of the patients respectively were free from combined endpoint. Five patients (20.8%) were readmitted with recurrent infective endocarditis.
Conclusion: In patients presenting with active intravenous drug abuse, treatment of infective endocarditis should be performed as aggressively as possible and should be followed by antibiotic therapy to avoid high mortality rates and recurrent endocarditis. Early intervention is advisable in patients with an infective endocarditis and enterococcus species in the preoperative blood cultures, liver function deterioration as well as cardiac function impairment. Attention should be also payed to addiction treatment, due to the elevated relapse rate in patients who actively inject drugs. However, larger prospective studies are necessary to support our results. As septic shock is the most frequent cause of death, new treatment options, e.g. blood purification should be evaluated.
Keywords: High risk valve procedures; Infective endocarditis; Intravenous drug abuse.
Conflict of interest statement
None declared.
Figures
References
-
- Degenhardt L, Peacock A, Colledge S, Leung J, Grebely J, Vickerman P, et al. Global prevalence of injecting drug use and sociodemographic characteristics and prevalence of HIV, HBV, and HCV in people who inject drugs: a multistage systematic review. Lancet Glob Heal. 2017;5(12):e1192–207. 10.1016/S2214-109X(17)30375-3. - PMC - PubMed
-
- Chu VH, Park LP, Athan E, Delahaye F, Freiberger T, Lamas C, et al. Association between surgical indications, operative risk, and clinical outcome in infective endocarditis a prospective study from the international collaboration on endocarditis. Circulation. 2015;131(2):131–140. doi: 10.1161/CIRCULATIONAHA.114.012461. - DOI - PubMed
-
- Moreillon P, Que YA. Lancet. 2004. Infective endocarditis. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
