

Which symptoms pose the highest risk in patients calling for an ambulance? A population-based cohort study from Denmark
- PMID: 33879211
- PMCID: PMC8056716
- DOI: 10.1186/s13049-021-00874-6
Which symptoms pose the highest risk in patients calling for an ambulance? A population-based cohort study from Denmark
Abstract
Background: Emergency medical service patients are a vulnerable population and the risk of mortality is considerable. In Denmark, healthcare professionals receive 112-emergency calls and assess the main reason for calling. The main aim was to investigate which of these reasons, i.e. which symptoms or mechanism of injury, contributed to short-term risk of death. Secondary aim was to study 1-30 day-mortality for each symptom/ injury.
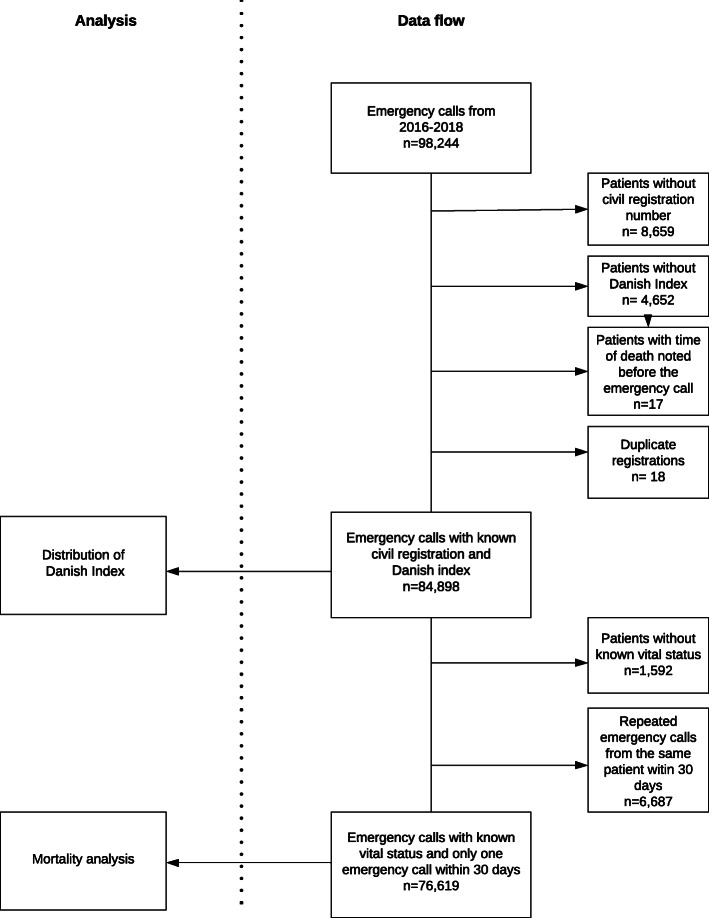
Methods: Historic population-based cohort study of emergency medical service patients calling 112 in the North Denmark Region between 01.01.2016-31.12.2018. We defined 1-day mortality as death on the same or the following day. The frequency of each symptom and cumulative number of deaths on day 1 and 30 together with 1- and 30-day mortality for each symptom/mechanism of injury is presented in proportions. Poisson regression with robust variance estimation was used to estimate incident rates (IR) of mortality with 95% confidence intervals (CI), crude and age and sex adjusted, mortality rates on day 1 per 100,000 person-year in the population.
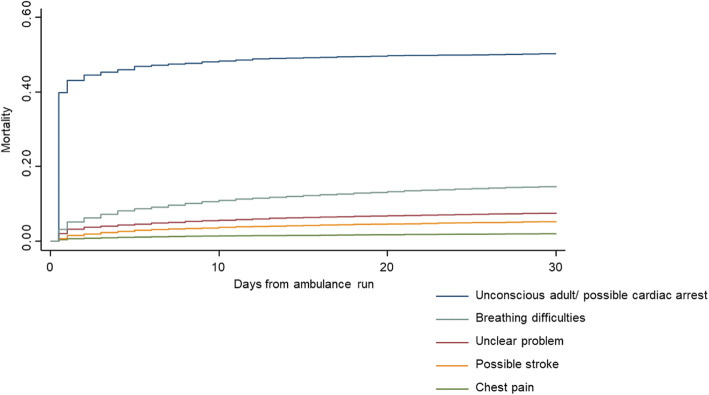
Results: The five most frequent reasons for calling 112 were "chest pain" (15.9%), "unclear problem" (11.9%), "accidents" (11.2%), "possible stroke" (10.9%), and "breathing difficulties" (8.3%). Four of these contributed to the highest numbers of deaths: "breathing difficulties" (17.2%), "unclear problem" (13.2%), "possible stroke" (8.7%), and "chest pain" (4.7%), all exceeded by "unconscious adult - possible cardiac arrest" (25.3%). Age and sex adjusted IR of mortality per 100,000 person-year was 3.65 (CI 3.01-4.44) for "unconscious adult - possible cardiac arrest" followed by "breathing difficulties" (0.45, CI 0.37-0.54), "unclear problem"(0.30, CI 0.11-0.17), "possible stroke"(0.13, CI 0.11-0.17) and "chest pain"(0.07, CI 0.05-0.09).
Conclusion: In terms of risk of death on the same day and the day after the 112-call, "unconscious adult/possible cardiac arrest" was the most deadly symptom, about eight times more deadly than "breathing difficulties", 12 times more deadly than "unclear problem", 28 times more deadly than "possible stroke", and 52 times more deadly than "chest pain". "Breathing difficulties" and "unclear problem" as presented when calling 112 are among the top three contributing to short term deaths when calling 112, exceeding both stroke symptoms and chest pain.
Keywords: Diagnosis; Emergency medical services; Emergency medicine; Mortality; Risk.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Christensen EF, Bendtsen MD, Larsen TM, Jensen FB, Lindskou TA, Holdgaard HO, et al. Trends in diagnostic patterns and mortality in emergency ambulance service patients in 2007–2014: a population-based cohort study from the North Denmark Region. BMJ Open. 2017;7(8):e014508. doi: 10.1136/bmjopen-2016-014508. - DOI - PMC - PubMed
-
- Dinh MM, Muecke S, Berendsen Russell S, Chalkley D, Bein KJ, Muscatello D, et al. Demand for emergency services trends in New South Wales years 2010–2014 (DESTINY): age and clinical factors associated with ambulance transportation to emergency departments. Prehosp Emerg Care. 2016;20(6):776–82. 10.1080/10903127.2016.1182603. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
