

Testing for non-inferior mortality: a systematic review of non-inferiority margin sizes and trial characteristics
- PMID: 33879485
- PMCID: PMC8061825
- DOI: 10.1136/bmjopen-2020-044480
Testing for non-inferior mortality: a systematic review of non-inferiority margin sizes and trial characteristics
Abstract
Objective: To describe the size and variability of non-inferiority margins used in non-inferiority trials of medications with primary outcomes involving mortality, and to examine the association between trial characteristics and non-inferiority margin size.
Design: Systematic review.
Data sources: Medline, Medline In Process, Medline Epub Ahead of Print and Embase Classic+Embase databases from January 1989 to December 2019.
Eligibility criteria: Prospective non-inferiority randomised controlled trials comparing pharmacological therapies, with primary analyses for non-inferiority and primary outcomes involving mortality alone or as part of a composite outcome. Trials had to prespecify non-inferiority margins as absolute risk differences or relative to risks of outcome and provide a baseline risk of primary outcome in the control intervention.
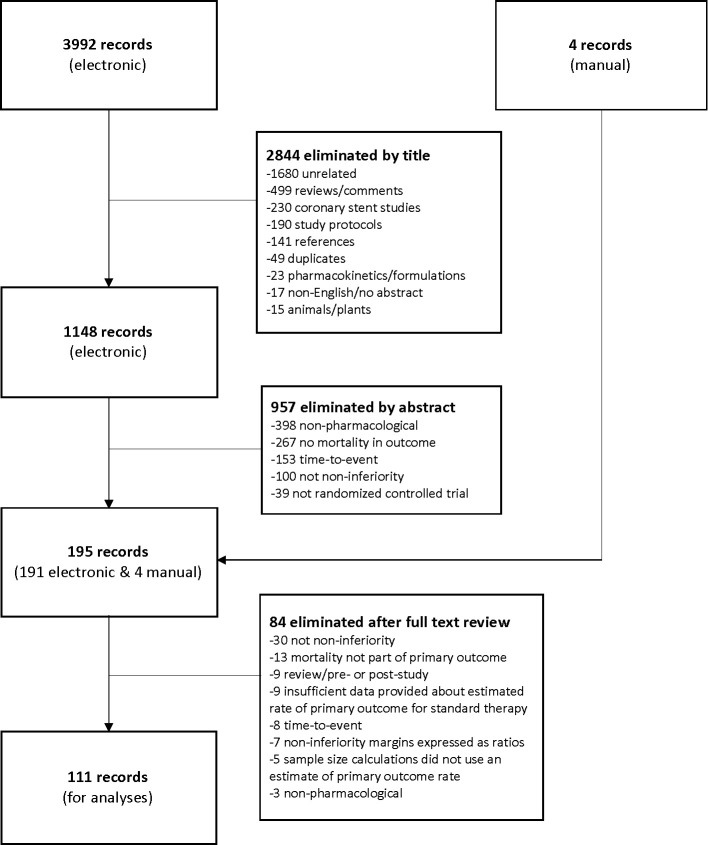
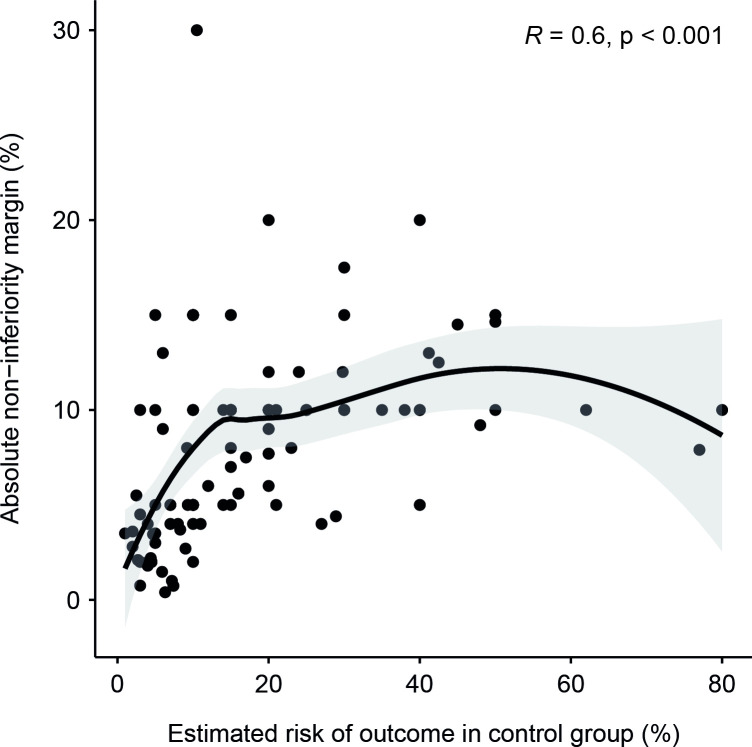
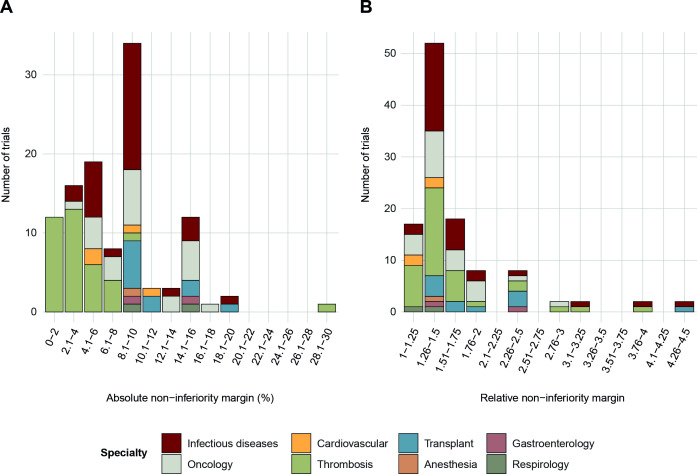
Results: 3992 records were screened, 195 articles were selected for full text review and 111 articles were included for analyses. 82% of trials were conducted in thrombosis, infectious diseases or oncology. Mortality was the sole primary outcome in 23 (21%) trials, and part of a composite primary outcome in 88 (79%) trials. The overall median non-inferiority margin was an absolute risk difference of 9% (IQR 4.2%-10%). When non-inferiority margins were expressed relative to the baseline risk of primary outcome in control groups, the median relative non-inferiority margin was 1.5 (IQR 1.3-1.7). In multivariable regression analyses examining the association between trial characteristics (medical specialty, inclusion of paediatric patients, mortality as a sole or part of a composite primary outcome, presence of industry funding) and non-inferiority margin size, only medical specialty was significantly associated with non-inferiority margin size.
Conclusion: Absolute and relative non-inferiority margins used in published trials comparing medications are large, allowing conclusions of non-inferiority in the context of large differences in mortality. Accepting the potential for large increases in outcomes involving mortality while declaring non-inferiority is a challenging methodological issue in the conduct of non-inferiority trials.
Keywords: clinical trials; epidemiology; statistics & research methods.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources