

Acquired hemophilia A associated with Epstein-Barr-virus-associated T/natural killer-cell lymphoproliferative disease: A case report
- PMID: 33879690
- PMCID: PMC8078394
- DOI: 10.1097/MD.0000000000025518
Acquired hemophilia A associated with Epstein-Barr-virus-associated T/natural killer-cell lymphoproliferative disease: A case report
Abstract
Introduction: Acquired hemophilia A (AHA) is a rare bleeding disorder caused by autoantibodies against factor VIII (FVIII). Hematological malignancies, especially lymphoid malignancies, are known to be underlying causes of AHA; however, thus far, there is no report of AHA associated with Epstein-Barr-virus-associated T/natural killer-cell lymphoproliferative disease (EBV-T/NK-LPD). Here, we present a case of AHA that developed during treatment for EBV-T/NK-LPD.
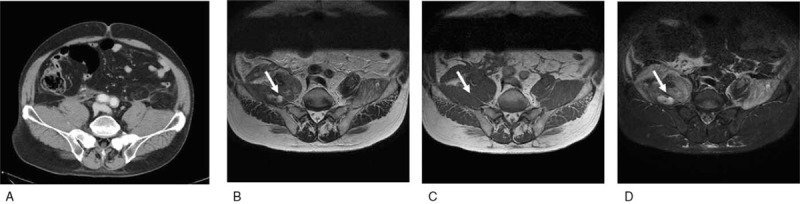
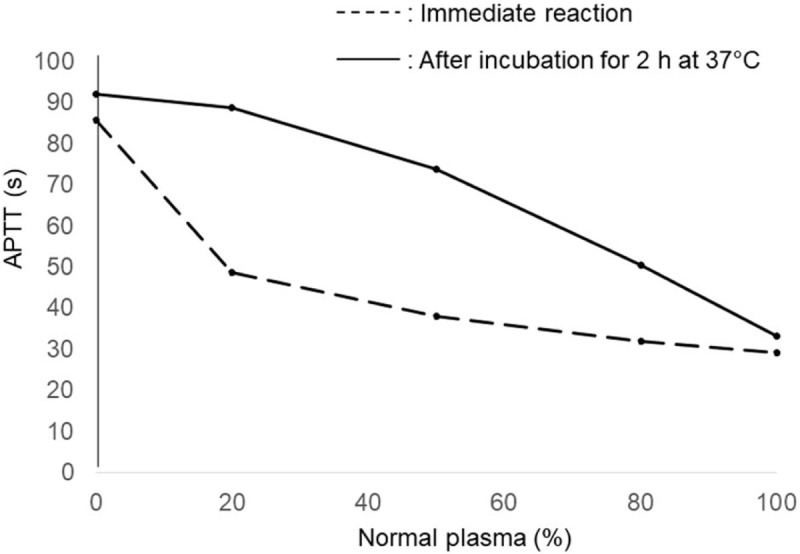
History: A 69-year-old man visited our hospital because of general fatigue. Blood examination showed pancytopenia, and computed tomography revealed whole-body lymphadenopathy, but there were no findings indicating hematological malignancy from bone marrow aspiration and cervical lymph node biopsy. The level of EBV DNA in peripheral blood was extremely high, and he was diagnosed with EBV-T/NK-LPD. EBV-T/NK-LPD improved with prednisolone (PSL) administration. Seventeen months after starting treatment, the patient complained of back and right leg pain. At that time, he had been treated with low-dose PSL, and EBV-T/NK-LPD was well controlled. Imaging revealed hematoma of the right iliopsoas muscle. Prolonged activated partial thromboplastin time (APTT) was the only abnormal finding in a screening coagulation test. FVIII coagulant activity was below detection limit, and FVIII inhibitor level was increased. From these results, he was diagnosed with AHA.A higher dose of PSL was administered, and, after 1 month of treatment, FVIII activity gradually increased, and FVIII inhibitor level became undetectable. APTT also normalized, and complete remission was achieved and maintained for 13 months with low-dose PSL. During treatment, EBV-T/NK-LPD was well controlled.
Conclusion: It is speculated that proliferating lymphocytes interfere with normal immune functions and that abnormal autoantibodies are produced from those lymphocytes in patients with LPD. Therefore, we speculate that EBV-infected and proliferating monoclonal NK cells might have modulated the immune system and produced autoantibodies against FVIII, thus causing AHA in this patient with EBV-T/NK-LPD.
Copyright © 2021 the Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
The authors have no funding and conflicts of interests to disclose.
Figures

Similar articles
-
Systemic Epstein-Barr virus positive T-cell lymphoproliferative disease of childhood with hemophagocytic syndrome.Int J Clin Exp Pathol. 2014 Sep 15;7(10):7110-3. eCollection 2014. Int J Clin Exp Pathol. 2014. PMID: 25400806 Free PMC article.
-
Central nervous system vasculitis from Epstein-Barr virus-associated T/natural killer-cell lymphoproliferative disorder in children: A case report.Brain Dev. 2019 Oct;41(9):820-825. doi: 10.1016/j.braindev.2019.05.009. Epub 2019 Jun 14. Brain Dev. 2019. PMID: 31208818
-
An adult case of systemic Epstein-Barr virus-positive T/natural killer-cell lymphoproliferative disorder with good outcome.Int J Clin Exp Pathol. 2013 Oct 15;6(11):2620-4. eCollection 2013. Int J Clin Exp Pathol. 2013. PMID: 24228130 Free PMC article.
-
Proposed categorization of pathological states of EBV-associated T/natural killer-cell lymphoproliferative disorder (LPD) in children and young adults: overlap with chronic active EBV infection and infantile fulminant EBV T-LPD.Pathol Int. 2008 Apr;58(4):209-17. doi: 10.1111/j.1440-1827.2008.02213.x. Pathol Int. 2008. PMID: 18324913 Review.
-
Chronic active Epstein-Barr virus infection of T-cell type, systemic form in an African migrant: case report and review of the literature on diagnostics standards and therapeutic options.BMC Cancer. 2018 Oct 3;18(1):941. doi: 10.1186/s12885-018-4861-0. BMC Cancer. 2018. PMID: 30285657 Free PMC article. Review.
References
-
- Fanchini M, Vaglio S, Marano G, et al. . Acquired hemophilia A: a review of recent data and new therapeutic opinions. Hematology 2017;22:514–20. - PubMed
-
- Kruse-Jarres R, Kempton CL, Baudo F, et al. . Acquired hemophilia A: updated review of evidence and treatment guidance. Am J Hematol 2017;92:695–705. - PubMed
-
- Fujiwara S, Kimura H, Imadome K, et al. . Current research on chronic active Epstein-Barr virus infection in Japan. Pediatr Int 2014;124:159–66. - PubMed
-
- Napolitano M, Siragusa S, Manccuso S, et al. . Acquired haemophilia in cancer: a systematic and critical literature review. Haemophilia 2018;24:43–56. - PubMed
-
- Sallah S, Nguyen NP, Abdallah JM, et al. . Acquired hemophilia in patients with hematologic malignancies. Arch Pathol Lab Med 2000;124:730–4. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
