

Robotic Hysterectomy for Benign Indications: What Have We Learned from a Decade?
- PMID: 33879990
- PMCID: PMC8035818
- DOI: 10.4293/JSLS.2020.00091
Robotic Hysterectomy for Benign Indications: What Have We Learned from a Decade?
Abstract
Background and objectives: Robotic surgery data need a setback on many years of practice with high-volume surgeons to evaluate its real value. Our main objective was to study the impact of a decade of robotic surgery on minimally-invasive hysterectomies for benign indications. Our secondary objectives were to evaluate our results for high-volume surgeons and complex cases.
Methods: In this retrospective cohort study, we reviewed medical records at Foch Hospital, from 2010 to 2019, to evaluate the outcomes of robotic hysterectomies for benign disease. We compared the trends of benign hysterectomies done by laparoscopy and laparotomy during this period. We analyzed the proficiency group (≥ 75 cases per surgeon) and complex cases including obese patients and large uteri (>250 g).
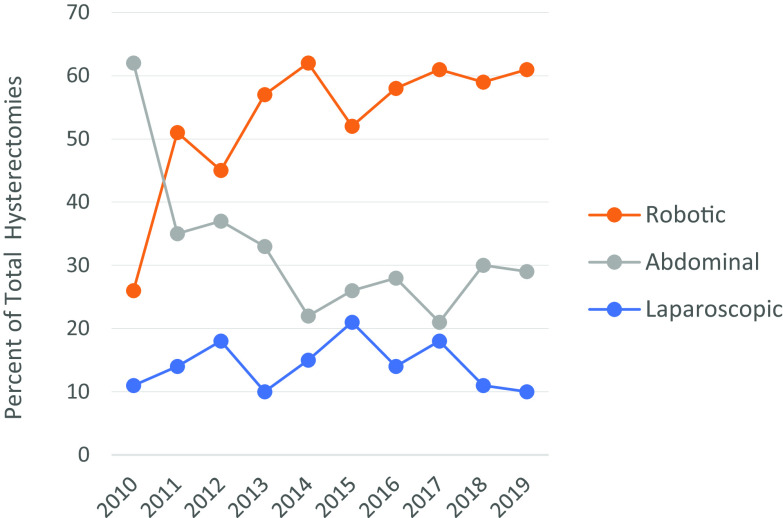
Results: 495 hysterectomies were performed by robotic, 275 by laparotomy, and 130 by laparoscopy. The laparotomy approach decreased from 62% to 29%, whereas the robotic approach increased from 26% to 61%. The operating room (OR) time decreased in the proficiency group (157.3 ± 43.32 versus 178.6 ± 48.05, P = 0.005); whereas the uterine weight was higher (194.6 ± 158.6 versus 161.3 ± 139.4, P = 0.04). Lower EBL and shorter OR time were seen with uteri ≤ 250 g subgroup (64.24 ± 110.2 ml versus 116.63 ± 146.98 ml, P = 0.0004) (169.62 ± 47.50 min versus 192.44 ± 45.82 min, P = 0.0001). The estimated blood loss (EBL) was less in the BMI ≤ 30 subgroup (68.83 ± 119.24 ml versus 124.53 ± 186.14 ml, P = 0.0005).
Conclusion: A shift was observed between the laparotomy and robotic approaches. High-volume surgeons were more efficient and showed a decrease in OR time after 75 cases despite an increase in uterine weight.
Keywords: Benign; Hysterectomy; Laparoscopy; Minimally invasive; Robotic-assisted.
© 2021 by SLS, Society of Laparoscopic & Robotic Surgeons.
Conflict of interest statement
Conflicts of interest: none.
Figures
References
-
- Garry R. Health economics of hysterectomy. Best Pract Res Clin Obstet Gynaecol. 2005;19(3):451–465. - PubMed
-
- Madhvani K, Curnow T, Carpenter T. Route of hysterectomy: a retrospective, cohort study in English NHS Hospitals from 2011 to 2017. BJOG. 2019;126(6):795–802. - PubMed
-
- ACOG Committee Opinion 444. Choosing the route of hysterectomy for benign disease. Obstet Gynecol. 2009;114(5):1156–1158. - PubMed
-
- Carbonnel M, Goetgheluck J, Frati A, Even M, Ayoubi JM. Robot-assisted laparoscopy for infertility treatment: current views. Fertil Steril. 2014;101(3):621–626. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical