

Impact of Frailty on the Risk of Exacerbations and All-Cause Mortality in Elderly Patients with Stable Chronic Obstructive Pulmonary Disease
- PMID: 33880018
- PMCID: PMC8053481
- DOI: 10.2147/CIA.S303852
Impact of Frailty on the Risk of Exacerbations and All-Cause Mortality in Elderly Patients with Stable Chronic Obstructive Pulmonary Disease
Abstract
Rationale: For the high prevalence of frail in patients with chronic obstructive pulmonary disease (COPD), further study should explore an in-depth understanding of the relationship between frailty and prognosis of COPD.
Objective: To determine the correlation between frailty and risk of acute exacerbation, hospitalizations, and mortality in older patients with stable COPD.
Participants and methods: Consecutive older adults (≥65) diagnosed with stable COPD from January 2018 to July 2019, with an average follow-up of 546 days (N = 309). Frailty was defined by the Fried frailty phenotype. Poisson regression was performed to assess the influence of frailty on the incidence of acute exacerbations of COPD (AECOPD) and all-cause hospitalizations in a year. Cox regression was performed to evaluate the effect of frailty on all-cause mortality in patients with stable COPD.
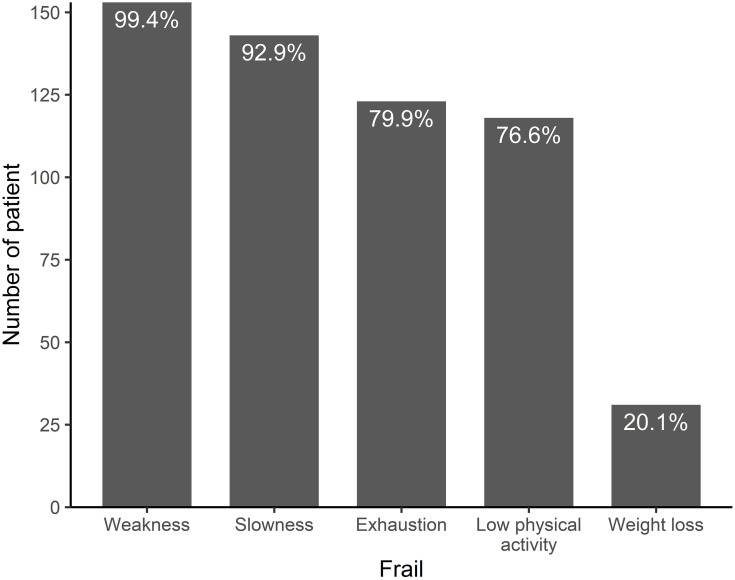
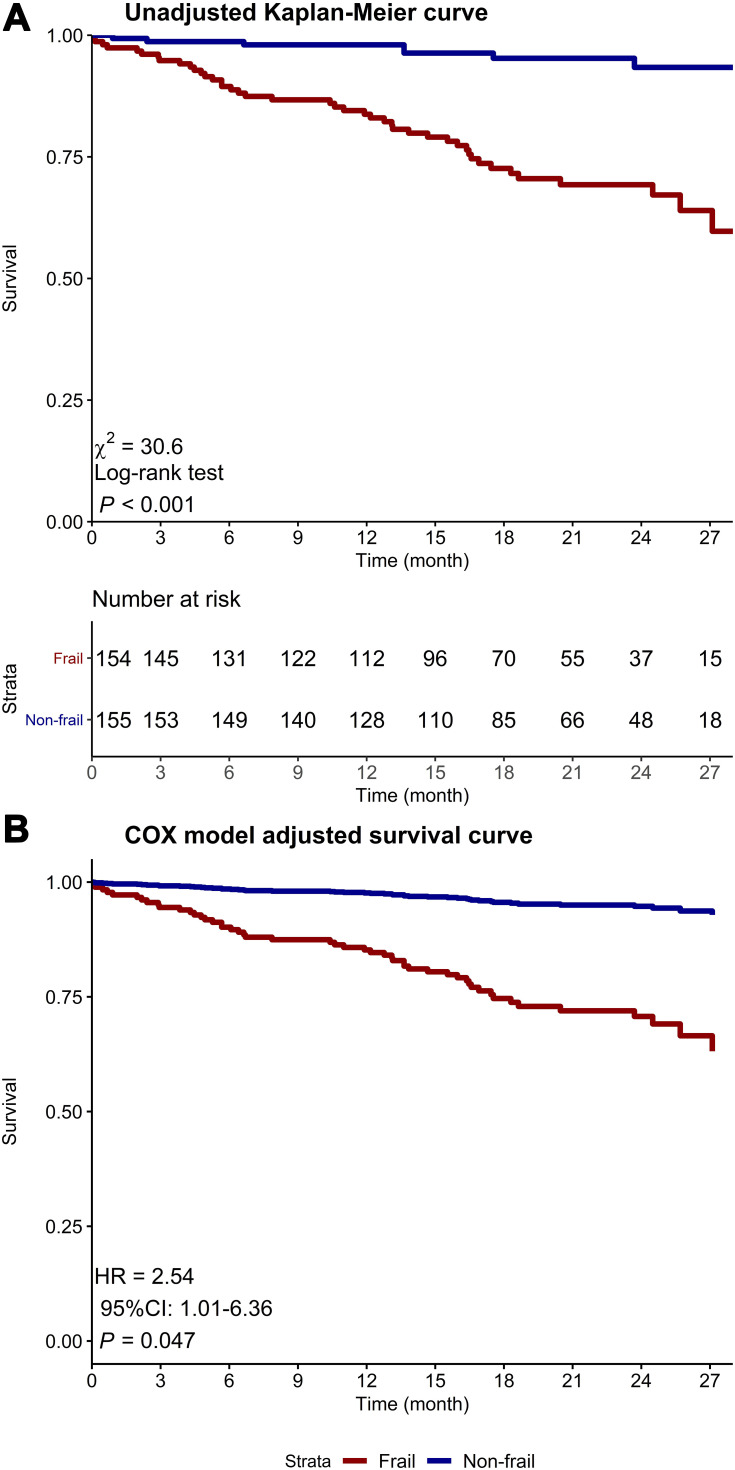
Results: The prevalence of frailty was 49.8%. The most common phenotypic characteristics were weakness (99.4%) followed by slowness (92.9%). After adjustment, frailty increased the incidence of AECOPD (IRR = 1.75, 95% CI: 1.09-2.82) and all-cause hospitalizations (IRR = 1.39, 95% CI 1.04-1.87) within a year. Slowness was associated with AECOPD (IRR = 1.77, 95% CI: 1.03-3.03), and weakness was associated with increased all-cause hospitalizations (IRR = 1.53, 95% CI: 1.04-2.25). The all-cause mortality risk was more than twofold higher in frail patients (HR = 2.54, 95% CI: 1.01-6.36) than non-frail patients. Low physical activity (HR = 2.66, 95% CI: 1.17-6.05) and weight loss (HR = 2.15, 95% CI: 1.02-4.51) were significantly associated with increased all-cause mortality in patients with COPD.
Conclusion: Frailty increased the incidence of acute exacerbation and hospitalization, as well as increased mortality in older patients with stable COPD. This knowledge will help physicians identify high-risk groups with COPD and frailty who may benefit from targeted interventions to prevent disease progression.
Keywords: COPD; acute exacerbation; frailty; mortality; older adults.
© 2021 Luo et al.
Conflict of interest statement
The authors report no conflicts of interest for this work.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
