

Original Article--Outcomes of Pacing in Egyptian Pediatric Population
- PMID: 33880330
- PMCID: PMC8051327
- DOI: 10.37616/2212-5043.1244
Original Article--Outcomes of Pacing in Egyptian Pediatric Population
Abstract
Objectives: Permanent pacemakers are widely used in the pediatric population due to congenital and surgically acquired rhythm disturbances. The diversity and complexity of congenital heart diseases make device management a highly individualized procedure in pediatric pacing. We are also faced with special problems in pediatric age group as growth, children's activity and infection susceptibility. This study aimed to present our institute's experience in pediatric and adolescent pacemaker implantation and long-term outcomes.
Methods: This cross-sectional observational study included 100 pediatric patients who visited our outpatient clinics at Ain Shams University Hospitals for regular follow up of their previously implanted permanent pacemakers. All patients were subjected to history taking, clinical examination, ECG recording, echocardiography and elaborate device programming. Data about device types, device components' longevity, subsequent procedures, complications were collected, with comparison between epicardial and endocardial pacemakers.
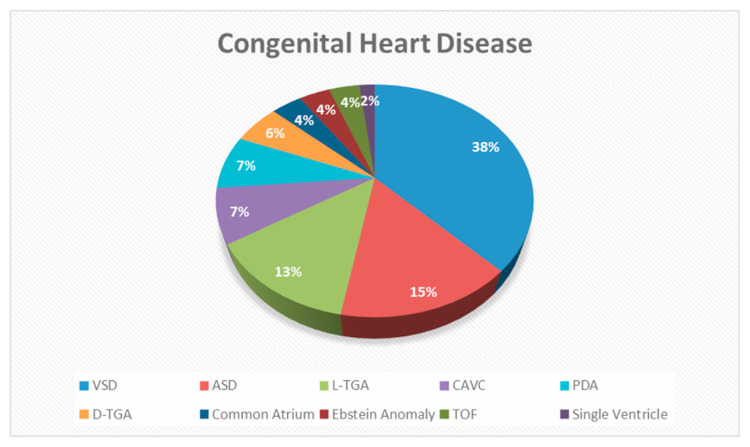
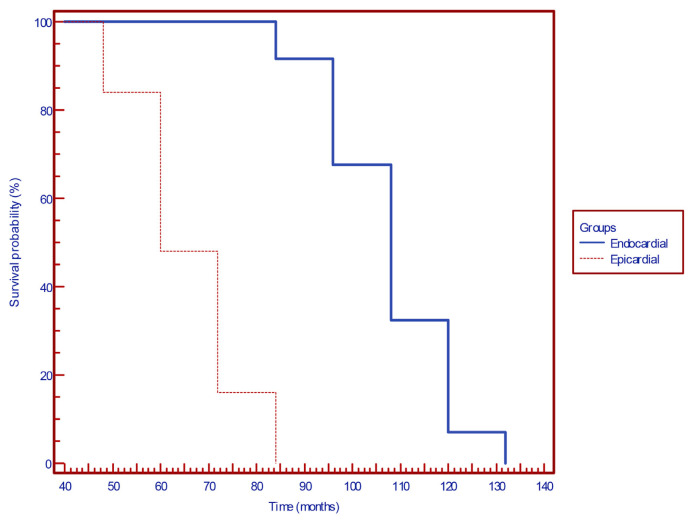
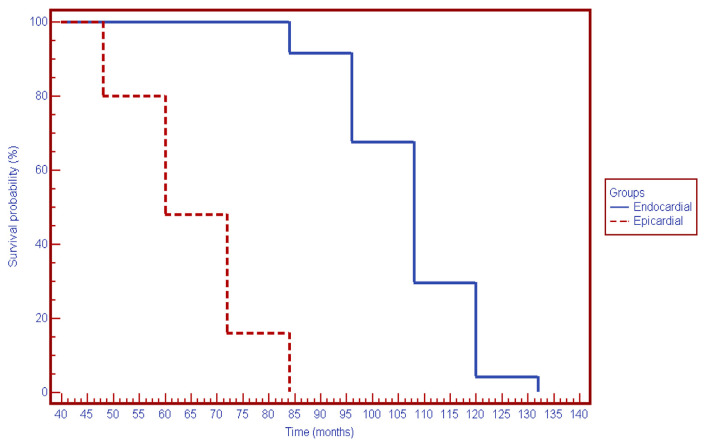
Results: Our study population ranged in age from 8 months to 18 years (mean 13.12 ± 5.04 years), 51 were males and 53 patients had congenital heart disease. Epicardial pacing represented 26% of our total population using only VVIR pacemakers, while endocardial pacing represented 74% of our population with 58.1% of them being VVIR pacemakers. First battery longevity was higher in endocardial batteries (108 months vs. 60 months, p value: 0.007). First lead longevity was also higher in endocardial leads (105 moths vs. 58 months, p value: 0.006). Complication rate was 25%; 8 patients had early complications (one insulation break in endocardial group). Late complications occurred in 17 patients (10 patients had lead fracture; 9 of them were endocardial, 2 insulation breaks in endocardial leads, 3 patients from epicardial group had lead failure of capture). In total, 16 patients had lead-related complications. There was no statistically significant difference between different lead models regarding lead-related complications.
Conclusion: Pacemakers in children are generally safe, but still having high rates of lead-related complications. Lead failure of capture was more common in epicardial leads. These complications had no relation to the model of the leads. Endocardial pacemakers showed higher first lead and first battery longevity compared to epicardial pacemakers.
Keywords: Endocardial pacing; Epicardial pacing; Pacing complications; Pediatric age; Permanent pacing.
© 2021 Saudi Heart Association.
Conflict of interest statement
Conflicts of interests All authors have none to declare.
Figures
Similar articles
-
Twenty years of paediatric cardiac pacing: 515 pacemakers and 480 leads implanted in 292 patients.Europace. 2006 Jul;8(7):530-6. doi: 10.1093/europace/eul062. Europace. 2006. PMID: 16798767
-
Long-term performance of bipolar epicardial atrial pacing using an active fixation bipolar endocardial lead.Pacing Clin Electrophysiol. 1998 May;21(5):1098-104. doi: 10.1111/j.1540-8159.1998.tb00156.x. Pacing Clin Electrophysiol. 1998. PMID: 9604242
-
Evaluation of different lead types and implantation techniques in pediatric populations with permanent pacemakers: Single-center with 10 years' experience.Pacing Clin Electrophysiol. 2021 Jan;44(1):110-119. doi: 10.1111/pace.14126. Epub 2020 Dec 1. Pacing Clin Electrophysiol. 2021. PMID: 33179296
-
Pacing device therapy in infants and children: a review.J Artif Organs. 2013 Mar;16(1):23-33. doi: 10.1007/s10047-012-0668-y. Epub 2012 Oct 27. J Artif Organs. 2013. PMID: 23104398 Review.
-
Efficacy of prophylactic epicardial pacing leads in children and young adults.Ann Thorac Surg. 2004 Jul;78(1):197-202; discussion 202-3. doi: 10.1016/j.athoracsur.2004.02.008. Ann Thorac Surg. 2004. PMID: 15223427 Review.
Cited by
-
Epicardial Versus Endocardial Pacing in Paediatric Patients with Atrioventricular Block or Sinus Node Dysfunction: A Systematic Review and Meta-analysis.Pediatr Cardiol. 2023 Dec;44(8):1641-1648. doi: 10.1007/s00246-023-03213-x. Epub 2023 Jul 22. Pediatr Cardiol. 2023. PMID: 37480376 Free PMC article.
References
-
- Beaufort-Krol GC, Mulder H, Nagelkerke D, Waterbolk TW, Bink-Boelkens MT. Comparison of longevity, pacing, and sensing characteristics of steroid-eluting epicardial versus conventional endocardial pacing leads in children. J Thorac Cardiovasc Surg. 1999 Mar;117(3):523–8. doi: 10.1016/s0022-5223(99)70332-6. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources