

Real-World Evidence for Control of Chronic Migraine Patients Receiving CGRP Monoclonal Antibody Therapy Added to OnabotulinumtoxinA: A Retrospective Chart Review
- PMID: 33880725
- PMCID: PMC8586140
- DOI: 10.1007/s40122-021-00264-x
Real-World Evidence for Control of Chronic Migraine Patients Receiving CGRP Monoclonal Antibody Therapy Added to OnabotulinumtoxinA: A Retrospective Chart Review
Abstract
Introduction: Combination use of onabotulinumtoxinA and calcitonin gene-related peptide (CGRP) monoclonal antibodies (mAbs) has the potential to be more effective than either therapy alone for migraine prevention.
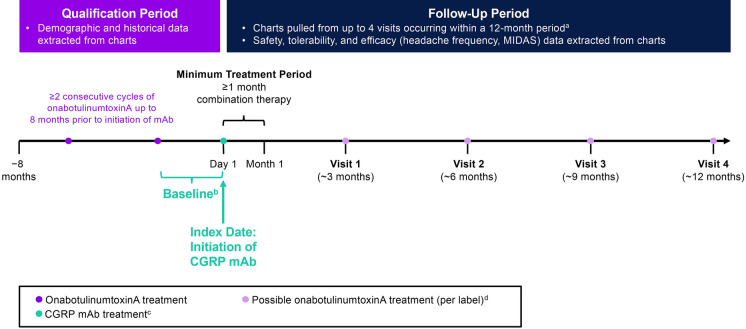
Methods: This retrospective, longitudinal chart review included adults with chronic migraine treated at one clinical site with ≥ 2 consecutive cycles of onabotulinumtoxinA and ≥ 1 month of subsequent combination treatment with CGRP mAbs. Charts at time of mAb prescription (baseline) and up to four visits ~ 3, 6, 9, and 12 months post-baseline were reviewed for safety, tolerability, and outcome measures (monthly headache days [MHDs], headache intensity, and migraine-related disability [MIDAS]).
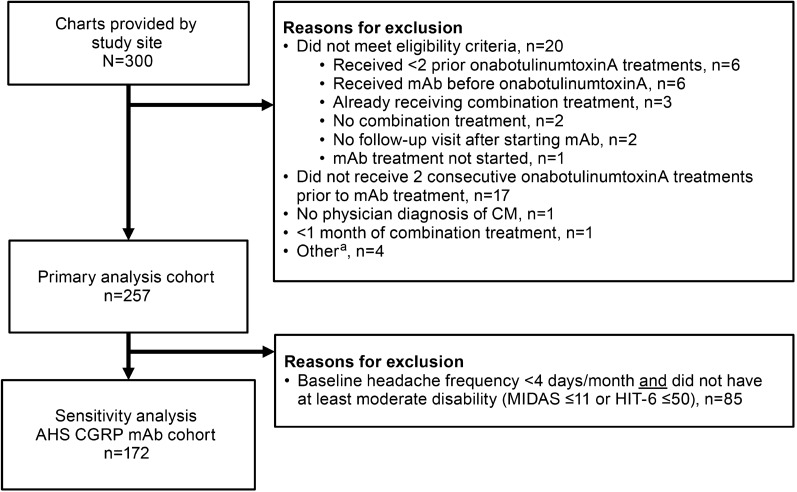
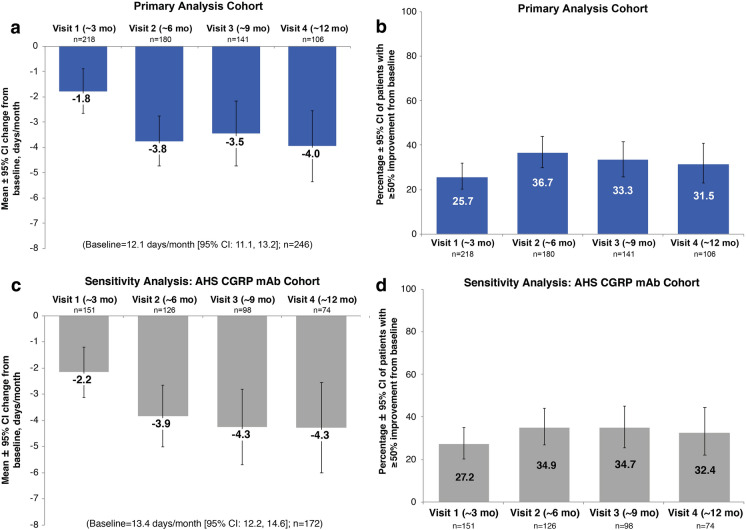
Results: Of 300 charts reviewed, 257 patients met eligibility criteria (mean age: 50 years; 82% women). Average headache frequency was 21.5 MHDs before initiation of onabotulinumtoxinA and 12.1 MHDs before adding CGRP mAb therapy. Prescribed mAbs were erenumab (78%), fremanezumab (6%), and galcanezumab (16%). Over the entire study, patients discontinued CGRP mAb more frequently than onabotulinumtoxinA (23 vs. 3%). Adverse events occurred in 28% of patients, most commonly constipation (9%). Compared with onabotulinumtoxinA alone (baseline), MHDs decreased significantly at all visits (mean decrease: 3.5-4.0 MHDs over ~ 6-12 months of combination treatment); 45.1% of patients had clinically meaningful improvement in migraine-related disability (≥ 5-point reduction in MIDAS score) after ~ 6 months.
Conclusions: In this real-world study, combination treatment with onabotulinumtoxinA and CGRP mAbs was well tolerated, with no new safety signals identified, and was associated with additional clinically meaningful benefits. More real-world and controlled trials should be considered to further assess safety and potential benefits of combination treatment. Video abstract: Real-world data suggests that CGRP inhibitors improve onabotulinumtoxinA efficacy for chronic migraine (MP4 20,067 kb).
Keywords: CGRP receptor; Chronic daily headache; Chronic headache; Combination therapy; Migraine headache; Preventive treatment; Type A botulinum toxins.
© 2021. The Author(s).
Figures

References
-
- IHS classification ICHD-3: migraine. 2019. https://ichd-3.org/1-migraine/. Accessed 18 Feb 2020.
-
- Lipton RB, Manack Adams A, Buse DC, Fanning KM, Reed ML. A comparison of the chronic migraine epidemiology and outcomes (CaMEO) study and American migraine prevalence and prevention (AMPP) study: demographics and headache-related disability. Headache. 2016;56:1280–1289. doi: 10.1111/head.12878. - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
