

Multilayered Human Skeletal Muscle Myoblast Sheets Promote the Healing Process After Colonic Anastomosis in Rats
- PMID: 33880968
- PMCID: PMC8076781
- DOI: 10.1177/09636897211009559
Multilayered Human Skeletal Muscle Myoblast Sheets Promote the Healing Process After Colonic Anastomosis in Rats
Abstract
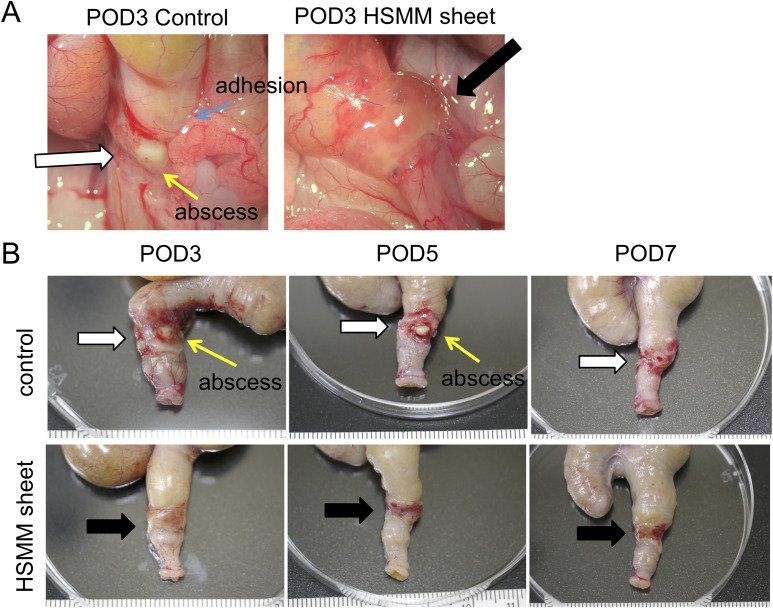
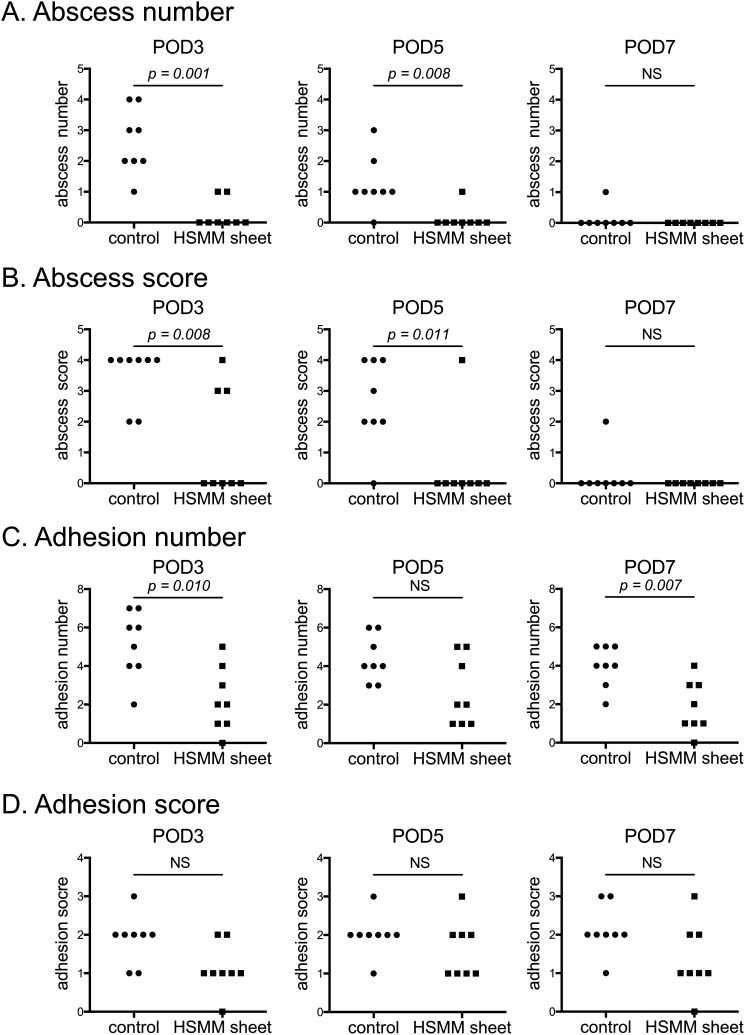
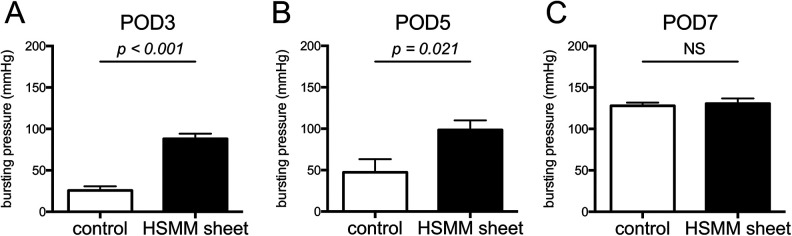
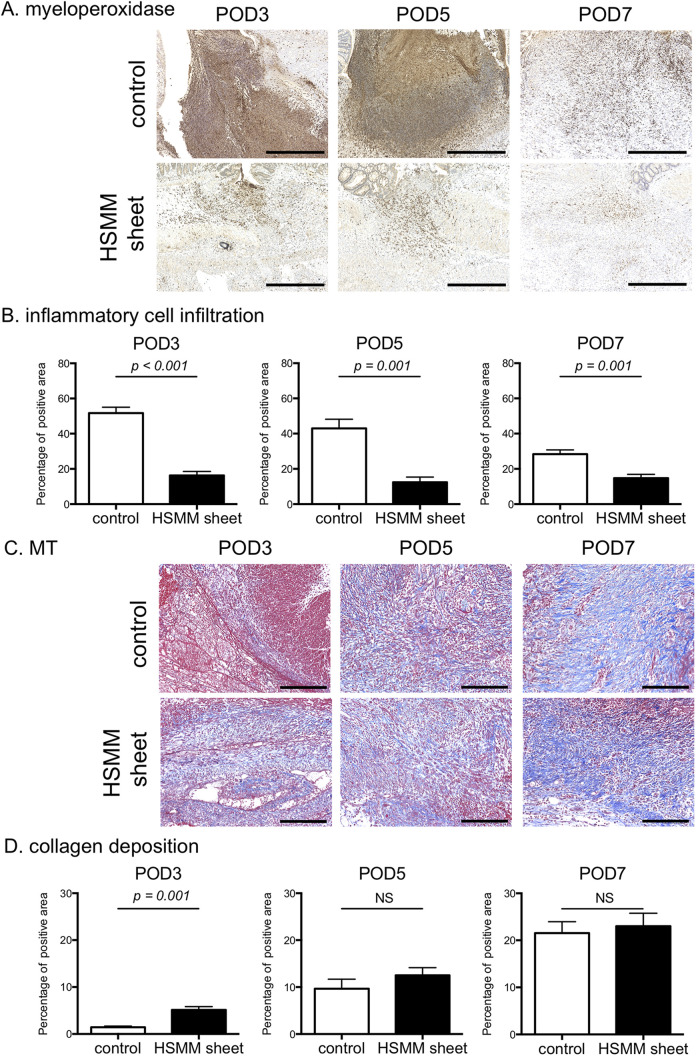
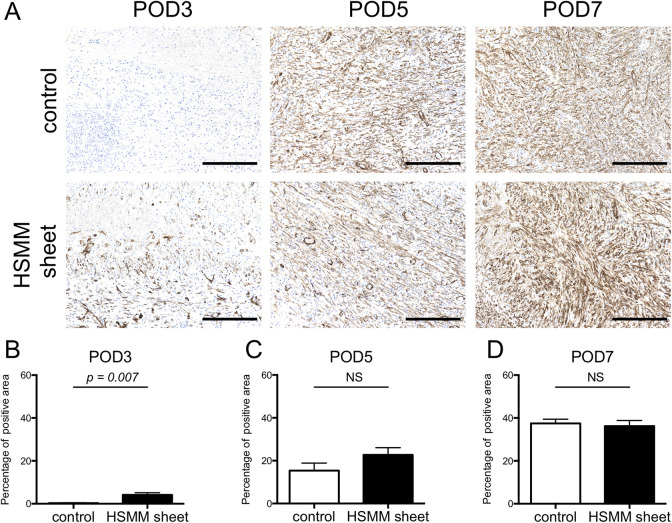
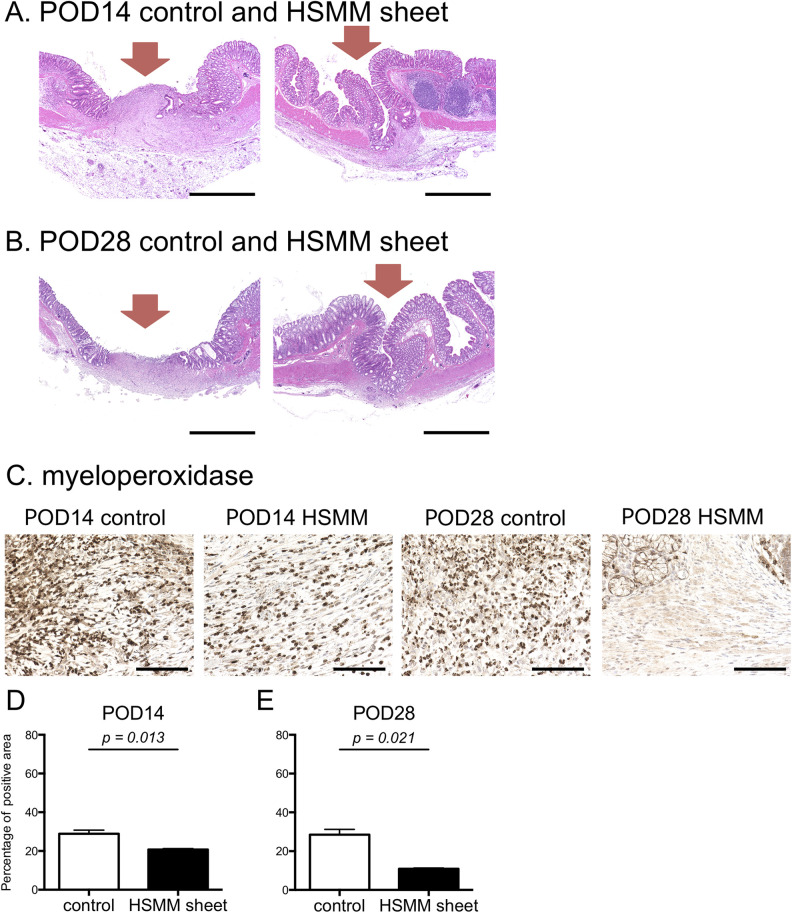
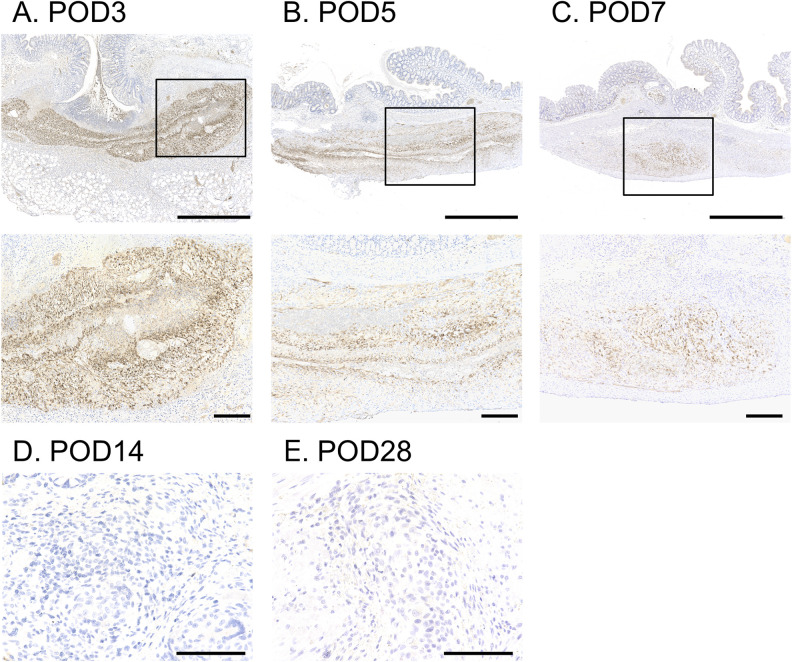
Colorectal anastomotic leakage is one of the most feared and fatal complications of colorectal surgery. To date, no external coating material that can prevent anastomotic leakage has been developed. As myoblasts possess anti-inflammatory capacity and improve wound healing, we developed a multilayered human skeletal muscle myoblast (HSMM) sheet by periodic exposure to supraphysiological hydrostatic pressure during repeated cell seeding. We assessed whether the application of an HSMM sheet can promote the healing process after colonic anastomosis. Partial colectomy and insufficient suturing were employed to create a high-risk colo-colonic anastomosis model in 60 nude rats. Rats were divided into a control group (n = 30) and an HSMM sheet group (n = 30). Macroscopic findings, anastomotic bursting pressure, and histology at the colonic anastomotic site were evaluated on postoperative day (POD) 3, 5, 7, 14, and 28. The application of an HSMM sheet significantly suppressed abscess formation at the anastomotic site compared to the control group on POD3 and 5. The anastomotic bursting pressure in the HSMM sheet group was higher than that in the control group on POD3 and 5. Inflammatory cell infiltration in the HSMM sheet group was significantly suppressed compared to that in the control group throughout the time course. Collagen deposition in the HSMM sheet group on POD3 was significantly abundant compared to that in the control group. Regeneration of the mucosa at the colonic anastomotic site was promoted in the HSMM sheet group compared to that in the control group on POD14 and 28. Immunohistochemical analysis demonstrated that surviving cells in the HSMM sheet gradually decreased with postoperative time and none were detected on POD14. These results suggest that the application of a multilayered HSMM sheet may prevent postoperative colonic anastomotic leakage.
Keywords: anastomotic leakage; hydrostatic pressure; mechanical stress; skeletal myoblast; tissue engineering.
Conflict of interest statement
Figures
References
-
- Vogel JD, Eskicioglu C, Weiser MR, Feingold DL, Steele SR. The american society of colon and rectal surgeons clinical practice guidelines for the treatment of colon cancer. Dis Colon Rectum. 2017;60(10):999–1017. - PubMed
-
- Kingham TP, Pachter HL. Colonic anastomotic leak: risk factors, diagnosis, and treatment. J Am Coll Surg. 2009;208(2):269–278. - PubMed
-
- Snijders HS, Wouters MW, van Leersum NJ, Kolfschoten NE, Henneman D, de Vries AC, Tollenaar RA, Bonsing BA. Meta-analysis of the risk for anastomotic leakage, the postoperative mortality caused by leakage in relation to the overall postoperative mortality. Eur J Surg Oncol. 2012;38(11):1013–1019. - PubMed
-
- Law WL, Choi HK, Lee YM, Ho JW, Seto CL. Anastomotic leakage is associated with poor long-term outcome in patients after curative colorectal resection for malignancy. J Gastrointest Surg. 2007;11(1):8–15. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
