

Family Genetic Risk Scores and the Genetic Architecture of Major Affective and Psychotic Disorders in a Swedish National Sample
- PMID: 33881469
- PMCID: PMC8060884
- DOI: 10.1001/jamapsychiatry.2021.0336
Family Genetic Risk Scores and the Genetic Architecture of Major Affective and Psychotic Disorders in a Swedish National Sample
Abstract
Importance: Family and genetic approaches have traditionally been used to evaluate our diagnostic concepts. Using a novel method, the family genetic risk score (FGRS), can we validate the genetic architecture of major affective and psychotic disorders in a national Swedish sample?
Objective: To determine whether FGRSs, calculated for the entire Swedish population, can elucidate the genetic relationship between major affective and psychotic disorders and clarify the association of genetic risk with important clinical features of disease.
Design, setting, and participants: This cohort study included the native Swedish population born from January 1, 1950, through December 31, 1995, and followed up through December 31, 2017. Data were collected from Swedish population-based primary care, specialist, and hospital registers, including age at first registration for a psychiatric diagnosis and number of registrations for major depression, bipolar disorder, and schizophrenia. Data were analyzed from October 15, 2020, to February 2, 2021.
Exposures: FGRSs for major depression, bipolar disorder, and schizophrenia calculated from morbidity risks for disorders in first- through fifth-degree relatives, controlling for cohabitation.
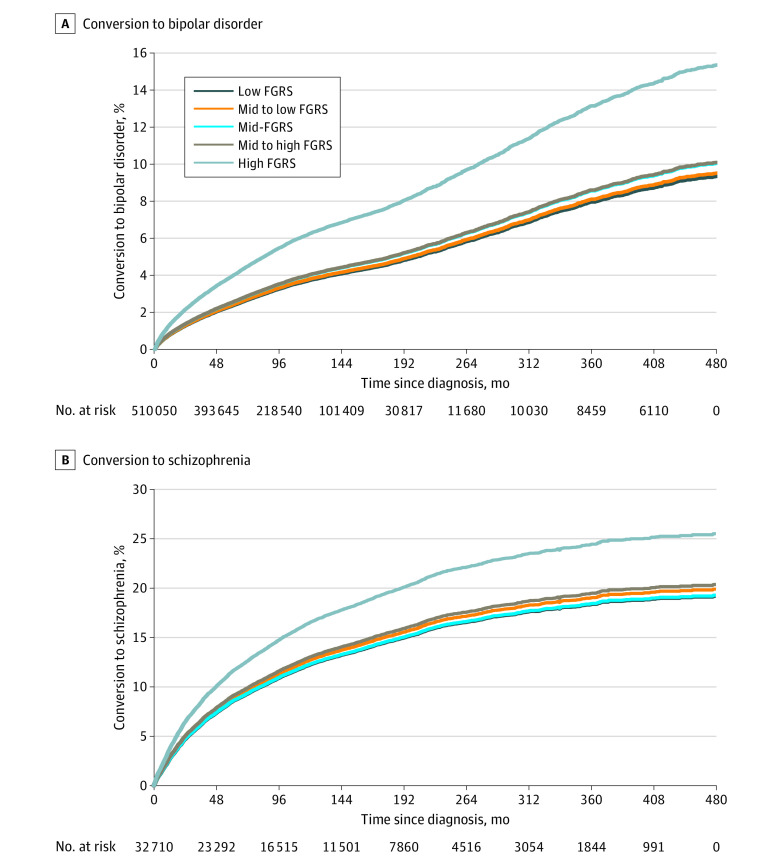
Main outcomes and measures: Diagnoses of major depression, bipolar disorder, schizophrenia, schizoaffective disorder, and other nonaffective psychoses (ONAPs), age at registration, and number of registrations for major depression, bipolar disorder, and schizophrenia. Diagnostic conversion of major depression to bipolar disorder and ONAPs to schizophrenia was assessed by Cox proportional hazards regression models.
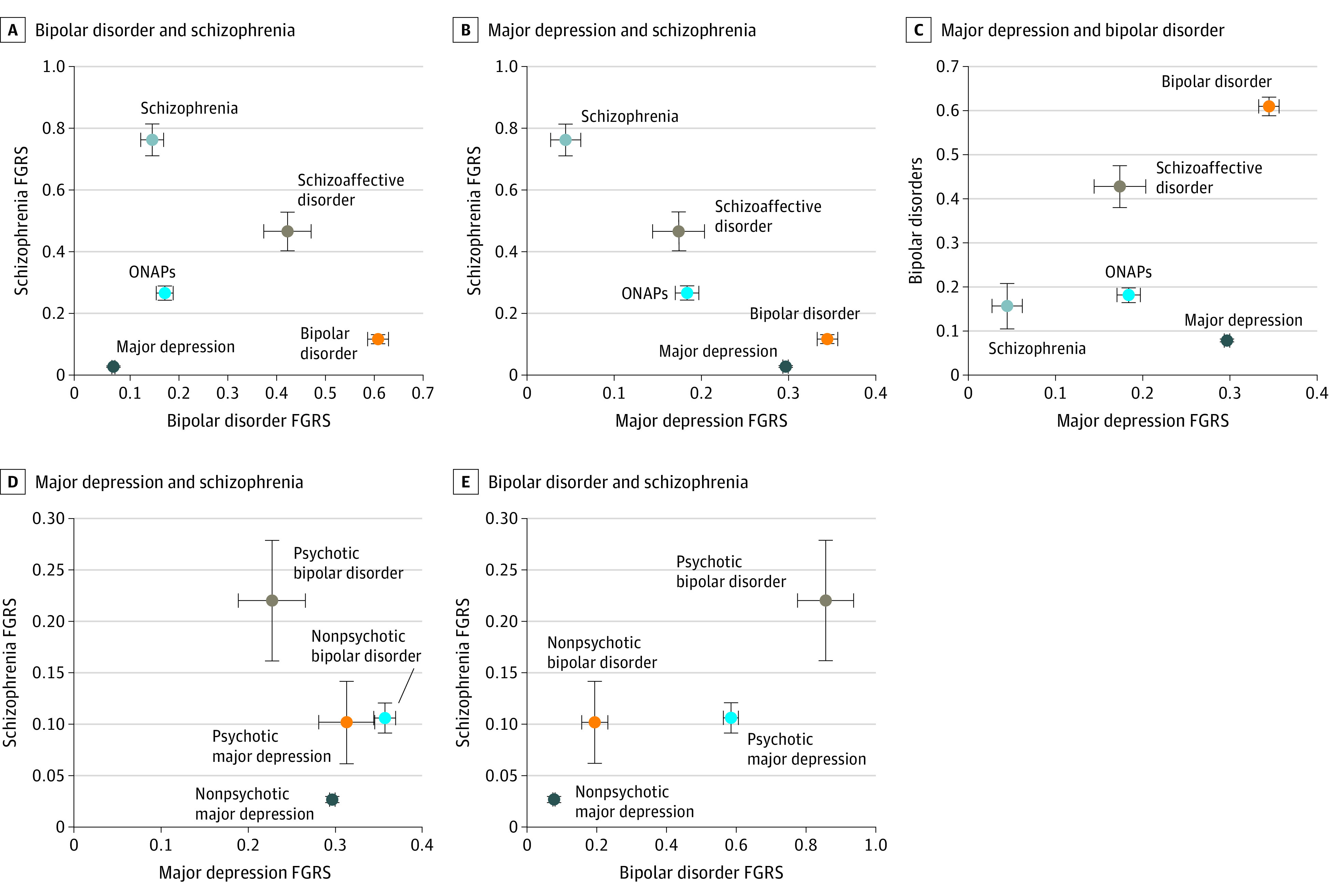
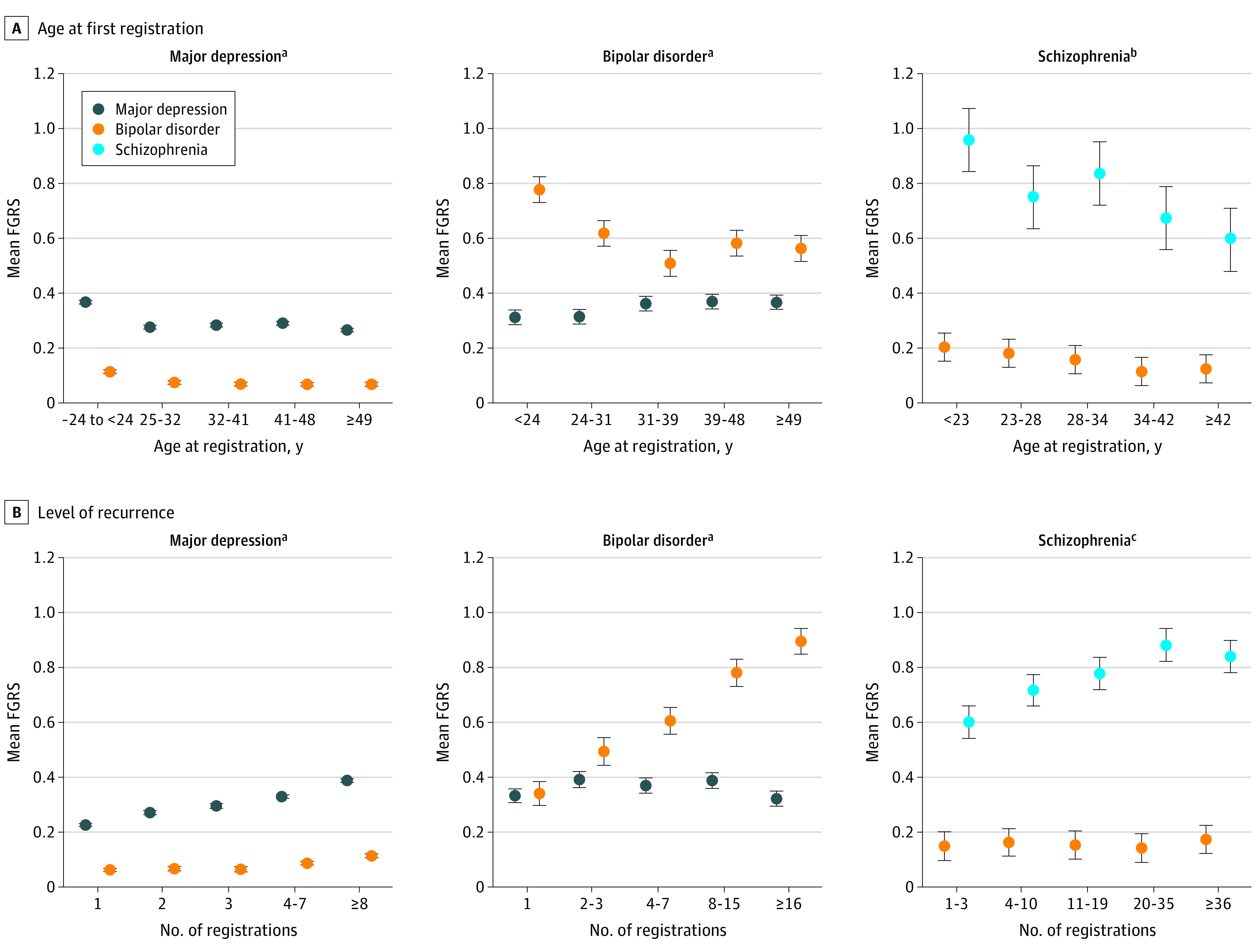
Results: The cohort included 4 129 002 individuals (51.4% male) with a mean (SD) age at follow-up of 45.5 (13.4) years. Mean FGRSs for major depression, bipolar disorder, and schizophrenia produced distinct patterns for major depression, bipolar disorder, schizophrenia, schizoaffective disorder, and ONAPs with large separations between disorders. In major depression, bipolar disorder, and schizophrenia, high FGRSs were associated with early age at onset and high rates of recurrence: a high mean FGRS for bipolar disorder was associated with early age at onset (younger than 25 years, 0.11; 95% CI, 0.11-0.12) and higher recurrence (8 or more registrations, 0.11; 95% CI, 0.11-0.12) in major depression. The schizophrenia FGRS was separately associated with psychotic and nonpsychotic forms of major depression (0.10; 95% CI, 0.06-0.14 vs 0.03; 95% CI, 0.02-0.03) and bipolar disorder (0.22; 95% CI, 0.16-0.28 vs 0.11; 95% CI, 0.09-0.12). The bipolar disorder and schizophrenia FGRSs were associated with conversion from major depression to bipolar disorder (eg, hazard ratio, 1.70 [95% CI, 1.63-1.78] for high vs low bipolar FGRS) and ONAP to schizophrenia (eg, hazard ratio, 1.38 [95% CI, 1.27-1.51] for high vs low schizophrenia FGRS).
Conclusions and relevance: In this Swedish cohort study, the FGRSs for major depression, bipolar disorder, and schizophrenia for the Swedish population clearly separated major affective and psychotic disorders from each other in a larger and more representative patient sample than previously possible. These findings provide possible validation, from a genetic perspective, for these major diagnostic categories. These results replicated and extended prior observations on more limited samples of the association of FGRS with age at onset, recurrence, psychotic subtypes, and diagnostic conversions.
Conflict of interest statement
Figures
References
-
- Kendler KS. The pre-history of psychiatric genetics: 1780-1910. Published online October 15, 2020. Am J Psychiatry.
-
- Tsuang MT, Faraone SV. The Genetics of Mood Disorders. Johns Hopkins University Press; 1990.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
