Effect of different thresholds for CT perfusion volumetric analysis on estimated ischemic core and penumbral volumes
- PMID: 33882098
- PMCID: PMC8059822
- DOI: 10.1371/journal.pone.0249772
Effect of different thresholds for CT perfusion volumetric analysis on estimated ischemic core and penumbral volumes
Abstract
Purpose: This single-center study compared three threshold settings for automated analysis of the ischemic core (IC) and penumbral volumes using computed tomographic perfusion, and their accuracy for predicting final infarct volume (FIV) in patients with anterior circulation acute ischemic stroke (AIS).
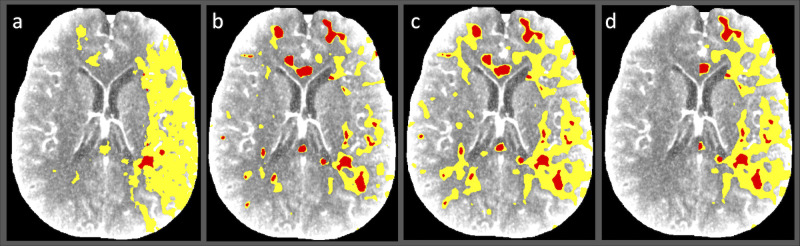
Methods: Fifty-two consecutive AIS patients undergoing mechanical thrombectomy (November 2015-March 2018) were included. Perfusion images were retrospectively analyzed using a single CT Neuro perfusion application (syngo.via 4.1, Siemens Healthcare GmbH). Three threshold values (S1-S3) were derived from another commercial package (RAPID; iSchema View) (S1), up-to-date syngo.via default values (S2), and adapted values for syngo.via from a reference study (S3). The results were compared with FIV determined by non-contrast CT.
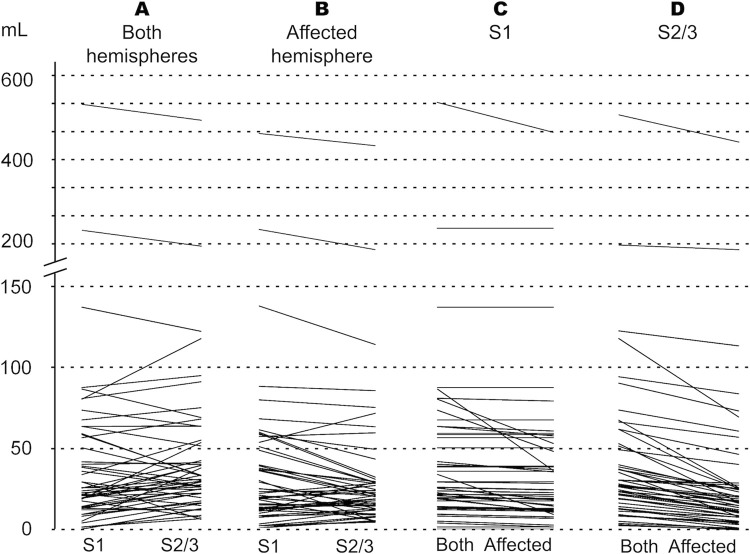
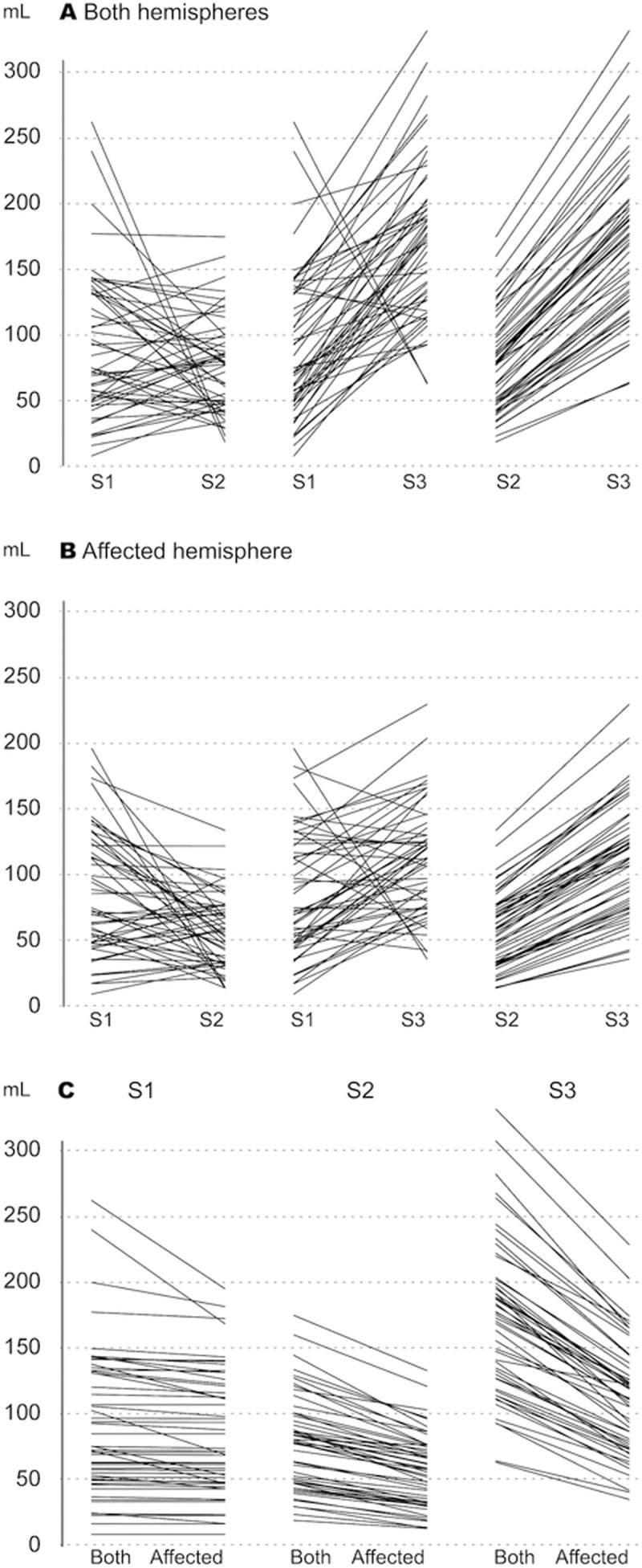
Results: The median IC volume (mL) was 24.6 (interquartile range: 13.7-58.1) with S1 and 30.1 (20.1-53.1) with S2/S3. After removing the contralateral hemisphere from the analysis, the median IC volume decreased by 1.33(0-3.14) with S1 versus 9.13 (6.24-14.82) with S2/S3. The median penumbral volume (mL) was 74.52 (49.64-131.91), 77.86 (46.56-99.23), and 173.23 (125.86-200.64) for S1, S2, and S3, respectively. Limiting analysis to the affected hemisphere, the penumbral volume decreased by 1.6 (0.13-9.02), 19.29 (12.59-26.52), and 58.33 mL (45.53-74.84) for S1, S2, and S3, respectively. The correlation between IC and FIV was highest in patients with successful recanalization (n = 34, r = 0.784 for S1; r = 0.797 for S2/S3).
Conclusion: Optimizing thresholds significantly improves the accuracy of estimated IC and penumbral volumes. Current recommended values produce diversified results. International guidelines based on larger multicenter studies should be established to support the standardization of volumetric analysis in clinical decision-making.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures